Figures & data
Figure 1 Baseline photograph at presentation in our scar clinic before initiation of combination therapy with cryotherapy directly followed by intralesional TAC (10 mg/mL) (A and B). Result after three cycles of combined cryo/intralesional TAC therapy before initiation of PDL (C). Result after four PDL applications (D). No signs of recurrence or reactivation at follow-up 6 months after the last laser treatment (E and F).
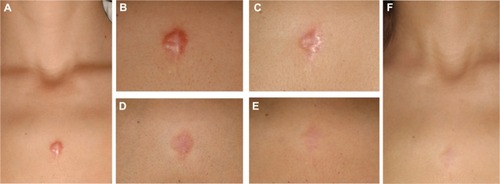
Figure 2 Patient with keloid in the presternal area resistant to cryotherapy and TAC, silicone gel sheeting, surgery and postoperative radiotherapy (recurrence) suffering from severe pruritus at baseline (A). Significant reduction of pruritus and flattening after 1 week of injection with 5-FU (50 mg/mL) and TAC (40 mg/mL), 3:1 (B). Result at 6 months after the last injection (two injections total), with no signs of recurrence, no pruritus (C).
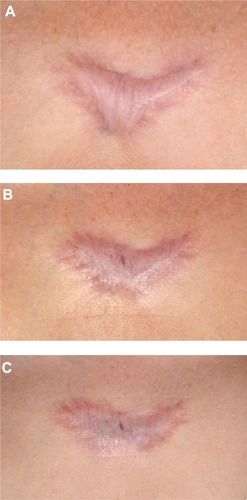
Figure 3 With intralesional cryotherapy, a specially designed cryoneedle is inserted (under translesional local anesthesia) into the long axis and mid height of the respective keloid.

Figure 4 Result at baseline (A and C) and after 3 and 6 years, respectively (B and D) post-intralesional cryotherapy.Adapted with permission from Har-Shai Y. Intralesional cryosurgery for enhancing the involution of hypertrophic scars and keloids. A new effective technology based on experimental and clinical data. Journal of wound Technology. 2012;15:8–9.Citation118
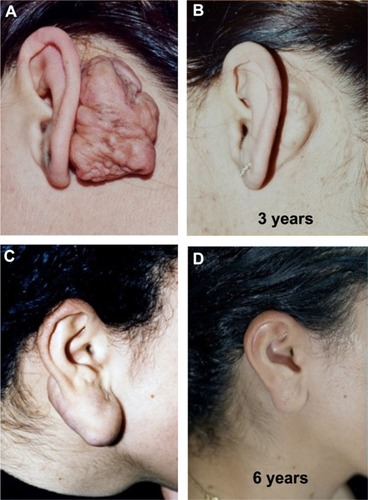
Table 1 Basic recommendations for the treatment of keloids and hypertrophic scars based on the experience of the author