Figures & data
Figure 1 Comparison of syringe-harvested isolated adipose-derived mesenchymal stromal cell (AD-MSC) counts (open circles) versus use of low-pressure machine harvest (wall suction or detuned lipoaspiration machine [dark circles]).
Abbreviation: OD, outside diameter.
![Figure 1 Comparison of syringe-harvested isolated adipose-derived mesenchymal stromal cell (AD-MSC) counts (open circles) versus use of low-pressure machine harvest (wall suction or detuned lipoaspiration machine [dark circles]).](/cms/asset/fb64aa63-8dce-4f73-b5a8-44cb9679b99a/dcci_a_40575_f0001_b.jpg)
Figure 2 Complete closed-syringe microcannula system (Tulip® GEMS™, Tulip Medical Systems, San Diego, CA, USA).

Figure 3 Tulip® super luer-lock connection (Tulip Medical Systems, San Diego, CA, USA).

Figure 4 Tulip® (Tulip Medical Systems, San Diego, CA, USA) cell-friendly (autoclavable) microcannulas.

Figure 5 Disposable microcannula cannulas for closed-syringe lipoaspiration of small-volume autologous adipose grafting (Tulip® GEMS™, Tulip Medical Systems, San Diego, CA, USA).

Figure 6 Close-up of microcannula openings.
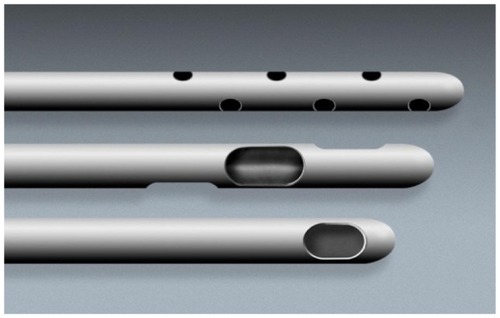
Figure 7 Closed-syringe lock options.

Figure 8 Anaerobic luer-to-luer transfer shown loading adipose graft to 1 cc treatment syringe.

Figure 9 Mechanical injector gun (Tulip®, Tulip Medical Systems, San Diego, CA, USA).
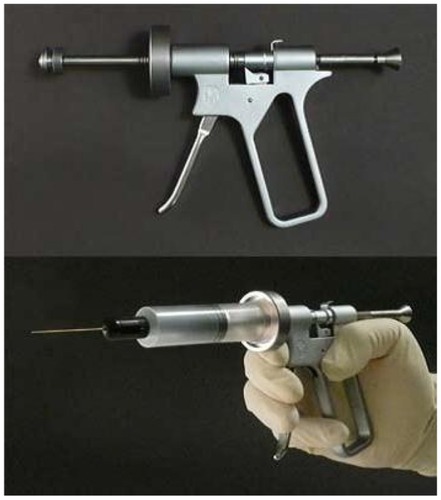
Figure 10 Example marking of lower abdomen site for harvesting of subdermal adipose tissue.

Figure 11 Placement of microcannula below Scarpa’s fascia in the adipose tissue plane.
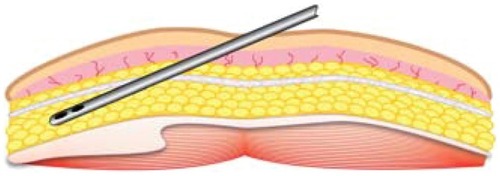
Figure 12 (A) Gravity decant base (luer); (B) gravity decant in test tube rack.
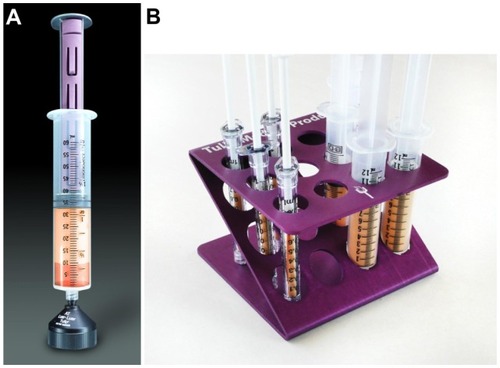
Figure 13 The SmartPRep®2 APC+™centrifuge, which forms part of the AdiPRep™ Adipose Transfer System (Harvest-Terumo, Plymouth, MA, USA).

Figure 14 Close-up of a disposable processing syringe containing extracted tissue that has separated.

Figure 15 Anaerobic transfer from disposable processing syringe (above) to adipose fat graft syringe (below).
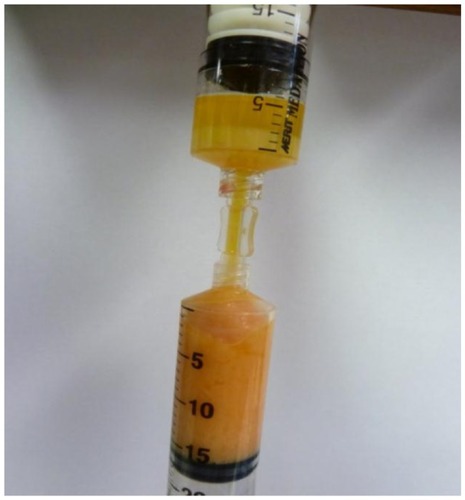
Figure 16 Tulip® GEMS™ (Tulip Medical Systems, San Diego, CA, USA) single-port injection cannulas (top) and close-up of the tip of one of these (bottom).

Figure 17 (A) Close-up of closed-cell compression foam (TenderFoam™; T&N Industries, San Diego, CA, USA). (B) Foam in place prior to firm compression.
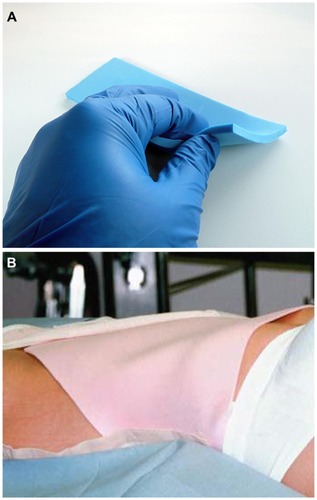
Figure 18 Clinical examples. Lips (A) pre- and (B) 1-year post-augmentation (autologous fat grafting [AFG] plus high-density platelet-rich plasma [HD PRP] [upper lip 3 cc; lower lip 2 cc]). (C) Pre- and (D) postoperative (20 months) AFG plus HD PRP grafting to lips, cheeks and nasolabial folds (lips: upper 2.5 cc; lower 2 cc; cheeks: 5 cc bilateral, malar and sub-malar placement; nasolabial folds: 3 cc bilateral). Cheeks (E and F) pre- and (G and H) 2 years post-AFG plus HD PRP (bilateral cheeks; total volume grafted, 5 cc bilateral malar and sub-malar) (Photos with permission). (I) Pre- and (J) postoperative (4 years) large-volume augmentation of both breasts (closed-syringe technique, cell-friendly cannulas) using AFG plus HD PRP concentrate; right, 300 cc; left, 325 cc).
![Figure 18 Clinical examples. Lips (A) pre- and (B) 1-year post-augmentation (autologous fat grafting [AFG] plus high-density platelet-rich plasma [HD PRP] [upper lip 3 cc; lower lip 2 cc]). (C) Pre- and (D) postoperative (20 months) AFG plus HD PRP grafting to lips, cheeks and nasolabial folds (lips: upper 2.5 cc; lower 2 cc; cheeks: 5 cc bilateral, malar and sub-malar placement; nasolabial folds: 3 cc bilateral). Cheeks (E and F) pre- and (G and H) 2 years post-AFG plus HD PRP (bilateral cheeks; total volume grafted, 5 cc bilateral malar and sub-malar) (Photos with permission). (I) Pre- and (J) postoperative (4 years) large-volume augmentation of both breasts (closed-syringe technique, cell-friendly cannulas) using AFG plus HD PRP concentrate; right, 300 cc; left, 325 cc).](/cms/asset/bbd7ced5-d61b-41aa-bd1e-bfb10064d16e/dcci_a_40575_f0018_c.jpg)