
Figures & data
Figure 1 Granulomatous mycosis fungoides. (A) Clinical features demonstrate multiple ill-defined erythematous indurated plaques on both legs, the lesion on the right leg showed large overlying ulceration. (B) Atypical lymphoid cell infiltrate with granulomatous reaction on histology (H&E x40) (inset, x400).
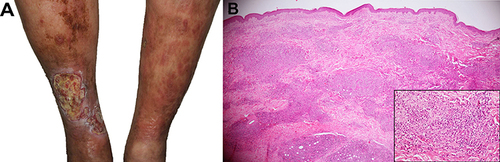
Figure 2 New round erythematous plaque on her right leg (A) and nodule on the left leg (B), measuring 2–3 cm in diameter with ulceration and central necrotic crust. The preexisting granulomatous mycosis fungoides shows large ulcerative brownish plaque on the distal leg (B).
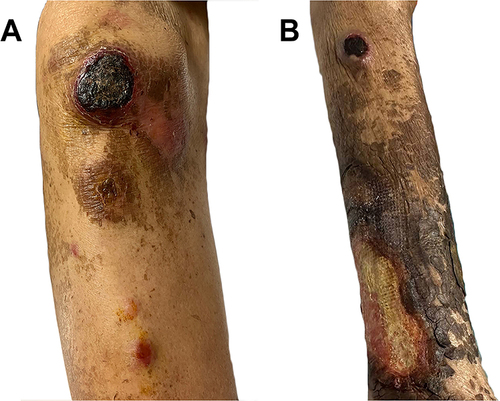
Figure 3 Histopathology from the new lesion on the left leg shows dense, diffuse atypical large mononuclear cell infiltration in the entire dermis (H&E x40); monomorphous atypical large lymphocytes of centroblastic morphology with frequent mitotic figures (inset, x400).
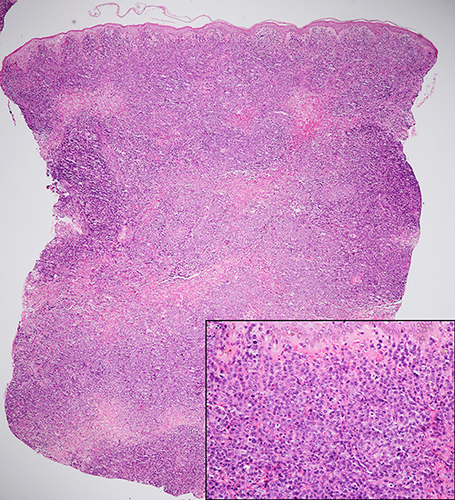
Figure 4 Immunohistochemistry of cutaneous methotrexate-related Epstein-Barr virus (EBV)-positive diffuse large B-cell lymphoma shows positive (A) CD20, (B) CD30, (C) Ki-67 (>90%), and (D) EBV encoded RNA by in situ hybridization (EBER-ISH) but negative (E) CD3 and (F) CD 56 staining of atypical lymphoid cells (H&E ×400).
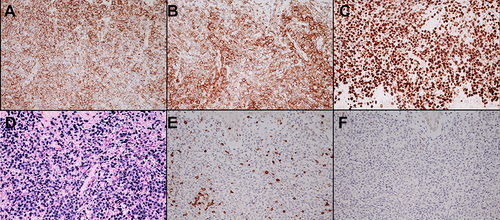
Table 1 Clinical and Laboratory Characteristics of Cutaneous Methotrexate-Related Diffuse Large B-Cell Lymphoma in the Patients with Known Cutaneous T-Cell Lymphoma