Figures & data
Table 1 Differential Diagnosis – Clinical Presentation – Imaging Modalities And Tissue Acquisition Techniques In Patients With MDBO
Figure 1 A 69-year-old presented with abdominal pain and cholestasis. MRI showed a double duct sign and a suspected lesion at the papillary area (A), presenting an abnormal diffusion-weighted signal and suggestive of an ampulloma (B). ERCP revealed an ampullary mass (C) and standard biopsies were performed confirming the diagnosis of ampullary carcinoma. A 10mm USEMS of 6 cm of length is placed to relieve the obstruction (D, E).
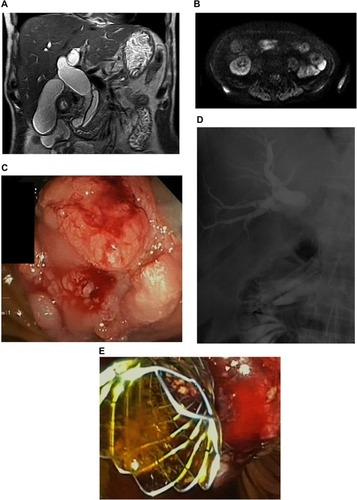
Figure 2 A 67-year-old woman presenting with dyspepsia, weight loss and jaundice. CT showed a 6 cm mass in the head of the pancreas with vascular involvement (SMV > 270°, SMA >120%) compressing the distal CBD (A). Both EUS-FNB and ERCP with brushings confirmed non-resectable pancreatic adenocarcinoma (B). A 10mm USEMS 4cm was inserted to provide drainage before neoadjuvant chemotherapy (C).

Figure 3 A 84-year-old woman presenting painless jaundice. TUS showed CBD and intrahepatic bile duct dilatation. MRI showed a suspected 22mm intraductal mass at the distal part of the CBD with an upstream dilatation (A). EUS-FNA confirmed an intraductal mass in the CBD suggestive of cholangiocarcinoma. ERCP revealed a long, irregular, distal biliary stricture (B); brushing and intraductal forceps biopsies confirmed the presence of malignant cells (C).
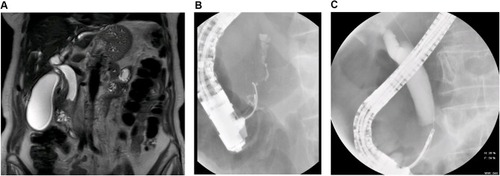
Figure 4 Algorithm for the assessment of patients with biliary obstruction.
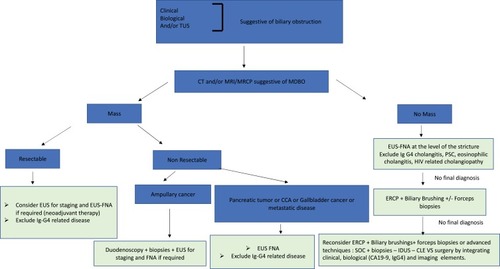
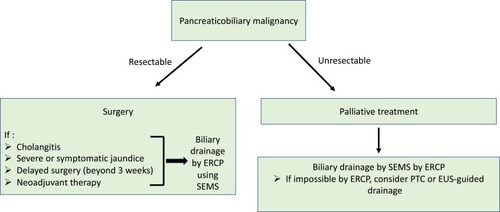
Figure 5 Algorithm for the endoscopic management of patients with confirmed pancreaticobiliary malignancy.