Figures & data
Figure 1 There was a mass near the cecum. The elevation of tissue fascia and free air were detected (A). There were several small polyps at ileocecal section (B).
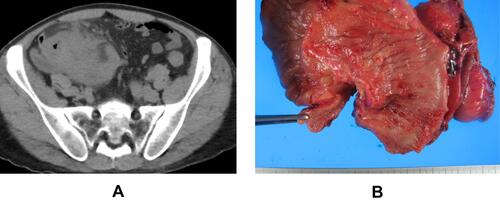
Figure 2 The enhanced CT in December 2017 showed the mass of 38mm with dyeing ring form in the left rectus abdominis muscle. The mass was located near the ileostomy closure scar. The triangle points to the tumor.

Figure 3 The MRI in April 2018 showed the mass of 40mm in the left rectus abdominis muscle. The mass showed low intensity area like muscle in T2 weighted images (A). It was uniformly enhanced (B). The triangle points to the tumor.
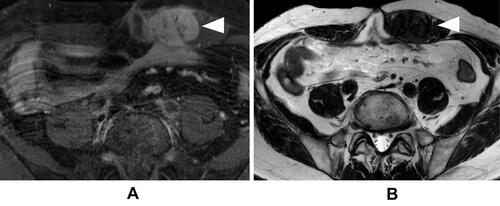
Figure 4 We performed a midline incision similar to the previous scar and we cut a spindle shape around the mass at 2cm margin from the mass (A). There was no exposure of the tumor to abdominal side. We used ultrasonically activated scalpel when we cut the muscle (B). Next, we removed the rectus abdominis muscle from the left lateral end. The abdominal wall defect was 10cm×10cm (C). The hernia was repaired with a simple closure using anterior layer of rectus sheath and the defect was closed by suturing the right anterior layer of rectus sheath to the left aponeurosis of external oblique muscle (D). We used a fascia lata patch measuring 15 cm × 5 cm (E) to repair the defect in the left abdomen (F).
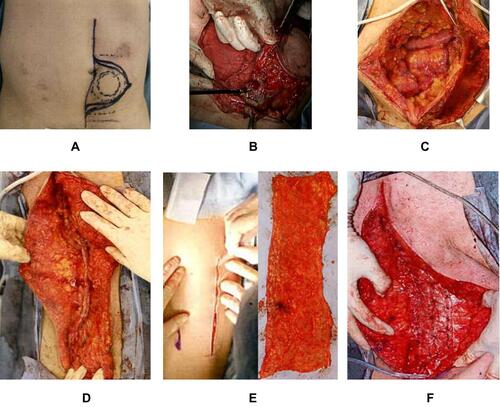
Figure 5 The final form after resection of tumor (A). The gray zone is the part that was removed. The defect was repaired with a simple closure and the defect was closed by suturing the right anterior layer of rectus sheath to the left aponeurosis of external oblique muscle (B). We used fascia lata patch as on lay mesh on defect (C).
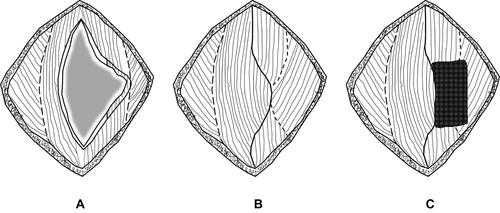
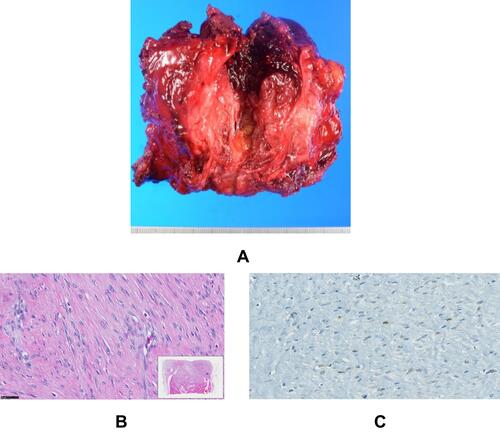
Figure 6 The tissue image is a magnified view of the red square part in the lower right image. The black line at the bottom left shows 50µm. The size of the mass was 45mm×45mm, the cut surface was white (A). The growth of fibroblasts was seen, the nuclear heteromorphic was poor. There was abundant collagen fibers between fibroblasts (B). A nuclear positive image of β-Catenin was observed by immunostaining (C).