Figures & data
Figure 1 Principle of the motility tracking system for evaluation of gut motility.
Notes: An elastic belt with detector is fixed to the patient’s abdomen. The magnetic capsule(s) is swallowed, and information about the position, direction, velocity, and amplitude of bowel movements can be recorded. When the capsule is expelled, data is extracted from the detector and segmental transit times can be calculated.
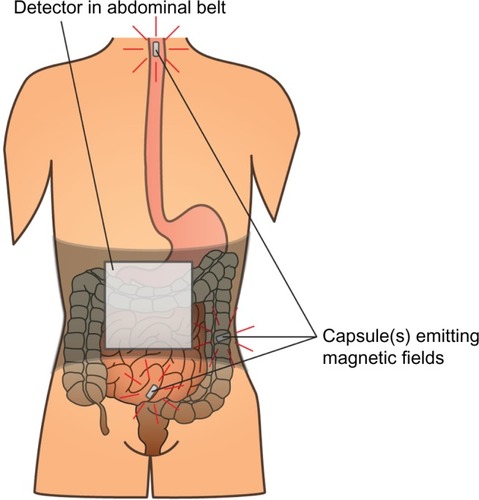
Figure 2 Schematic representation of the Ussing chamber measuring gut secretion.
Notes: Viable biopsies are mounted between two chambers filled with Krebs-Ringer solution. The two chambers respectively simulate blood stream and gut lumen. The mounted intestinal mucosa actively pumps ions from one chamber to the other and the resultant electrical gradient between chambers is measured with electrodes inserted on both sides.
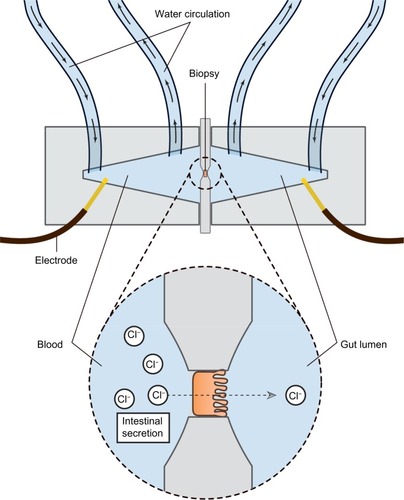
Figure 3 The FLIP probe.
Notes: The balloon is placed in the anal sphincter and filled with saline water. Through 16 electrodes the cross-sectional area and pressure can be monitored real-time and recorded, which can be used to derive the geometric profile of the sphincter function both during relaxation and challenge-testing.
Abbreviation: FLIP, functional lumen imaging probe technique.
Abbreviation: FLIP, functional lumen imaging probe technique.
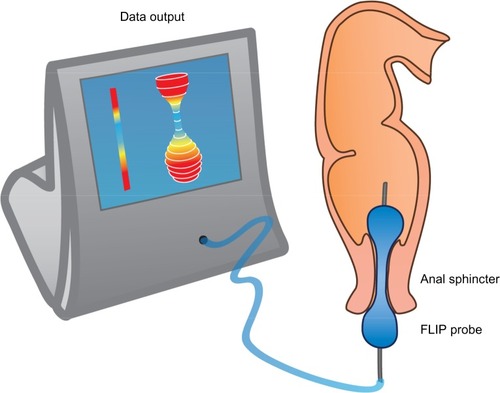
Table 1 Underlying mechanisms, symptoms, and the potential effects of PAMORAs and laxatives, respectively
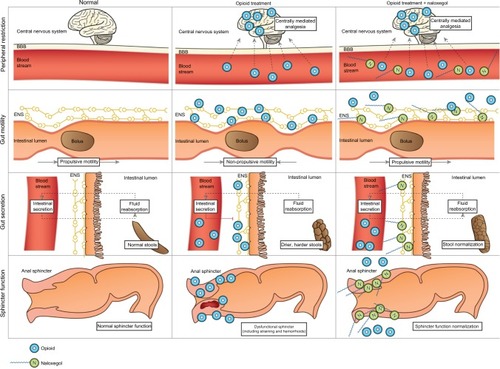
Figure 4 Pharmacological principle of naloxegol under normal conditions (left column), during opioid treatment (middle) and opioid and naloxegol treatment (right).
Notes: First row: opioids in the systemic circulation cross the blood–brain barrier and induce analgesia. Peripheral restriction prevents naloxegol from crossing the blood–brain barrier, thus centrally mediated analgesia is maintained. Second row: opioids bind to enteric nervous system μ-opioid receptors and cause non-propulsive motility. Due to higher affinity, naloxegol displaces opioids from the receptors in the gut and thus prevents dysmotility. Third row: naloxegol antagonizes the decreased secretion of electrolytes and water to the intestinal lumen, which results in a less dry, softer stool. Fourth row: in the gastrointestinal sphincters (here illustrated by the anal sphincter), naloxegol (at least theoretically) prevents sphincter dyscoordination and increased resting tone, with a net result of less straining and easier evacuation.
Abbreviations: ENS, enteric nervous system; BBB, blood–brain barrier.
Abbreviations: ENS, enteric nervous system; BBB, blood–brain barrier.