
Figures & data
Figure 1 Decision tree component of the model.
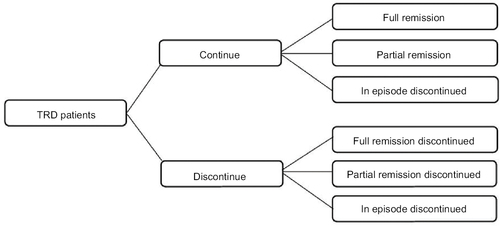
Figure 2 Markov component of the model.
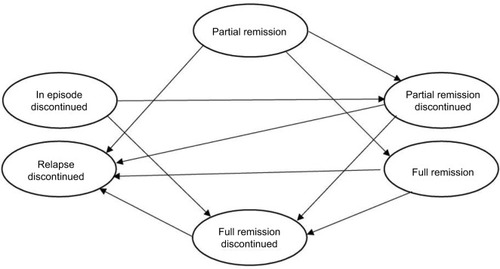
Table 1 Summary of treatment-specific model inputs
Table 2 Summary of treatment-unspecific model inputs
Table 3 Simulated acute treatment efficacy
Table 4 Base case model results
Figure 3 Deterministic sensitivity analysis on INMB at WTP of £30,000 per QALY for the hypothetical monotherapy with both efficacy and tolerability advantages.
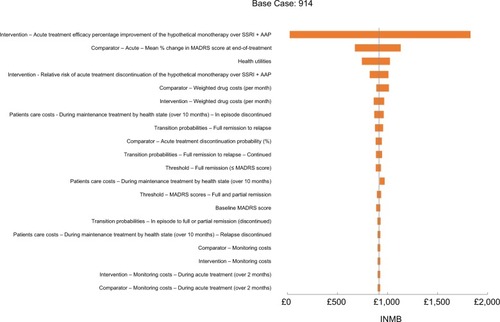
Figure 4 Cost-effectiveness plane for the hypothetical monotherapy with both efficacy and tolerability advantages.
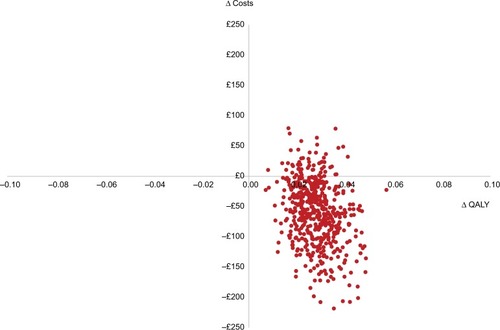
Figure 5 Cost-effectiveness acceptability curves for the hypothetical monotherapy with both efficacy and tolerability advantages.
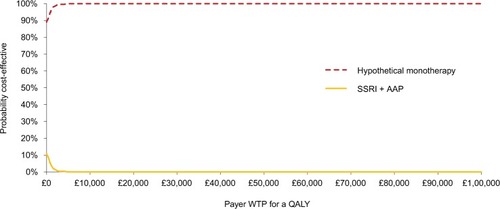
Figure 6 Combinations of acute treatment discontinuation and efficacy percentage advantages over SSRI + AAP that result in dominance of the hypothetical monotherapy (lower costs and higher QALYs).
Abbreviations: AAP, atypical antipsychotics; QALYs, quality-adjusted life years; SSRI, selective serotonin reuptake inhibitors.
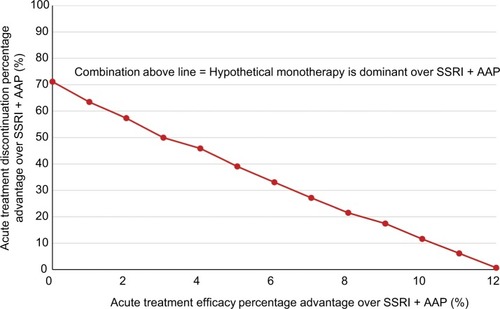
Table S1 Commonly prescribed drugs and the weighted monthly costs used in the model
Table S2 ICUR of the hypothetical monotherapy for different combinations of acute treatment discontinuation and efficacy percentage advantages over SSRI + AAP
Table S3 Optimal monthly prices of the hypothetical monotherapy for different combinations of acute treatment discontinuation and efficacy percentage advantages over SSRI + AAP at WTP per QALY of £30,000