
Figures & data
Figure 1 (A–D) A procedure has earlier been described by the group when implanting a permanent peritoneal PleurX catheter.Citation18
Notes: The procedure is here briefly described for the implantation of a pleural PleurX catheter performed in local anesthesia (Xylocaine 1%) and under sterile conditions using the PleurX catheter kit (A). Two skin incisions are made, one medial for guide wire insertion and one ~5–8 cm lateral and caudal to the first incision for catheter exit. The fenestrated end of a 15.5-G pleural catheter is tunneled subcutaneously from the caudal lateral to the cranial medial incision crossing the costophrenic sulcus (B). Under US guidance, a J-Tip guide wire is inserted into the pleural space by an 18-G needle through the inferior incision. The needle is removed and a 16-G peel-away introducer is passed over the guide wire, and the guide wire is removed (C). The subcutaneously placed fenestrated end of the catheter is inserted into the peel-away introducer and further into the pleural space, and the peel-away introducer is removed. Both incisions are sutured. The catheter is sutured to the skin (D), connected to the catheter bag, and opened to ensure flow. Bandages are applied.
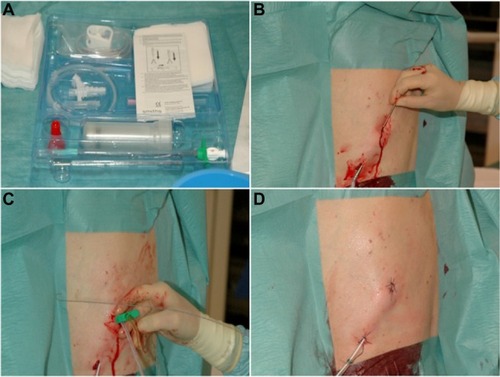
Table 1 Descriptive characteristics of 18 consecutive patients who had a permanent PleurX catheter implanted because of recurrent MPE
Table 2 Procedure-related AEs in 18 consecutive patients who had a permanent PleurX catheter implanted because of recurrent MPE