Figures & data
Table 1 Clinical characteristics of the 73 patients with colorectal cancer
Table 2 Patients with colorectal cancer having increased HER2 copy number
Figure 1 HER2 expression and copy number alterations in colorectal cancer (CRC). (A) Copy number (CN) alterations in the 73 CRCs included herein were analyzed using the Oncomine Comprehensive Assay. Red and blue circles represent HER2-positive and -negative CRCs, respectively, as determined using the HERACLES Diagnostic Criteria. (B) A representative histologic section of HER2-positive CRC showed moderately differentiated adenocarcinoma with a disoriented arrangement and confluent glandular structures (left). IHC staining with anti-HER2 antibody revealed intense (3+) HER2 expression (middle), while FISH analysis showed HER2 amplification with a HER2/CEN17 ratio of 6.26 (right). (C) A representative Hematoxylin and Eosin staining of HER2-negative CRC (left) with 0+ HER2 IHC staining (middle) and a non-amplified HER2/CEN17 ratio of 1.45 (right). (D) HER2 mRNA expression in 193 CRCs obtained from the TCGA database was analyzed. Putative copy number alterations were estimated using the Genomic Identification of Significant Targets In Cancer (GISTIC) algorithm. Red and blue circle represent HER2-amplified and HER2-nonamplified CRCs determined using GISTIC.
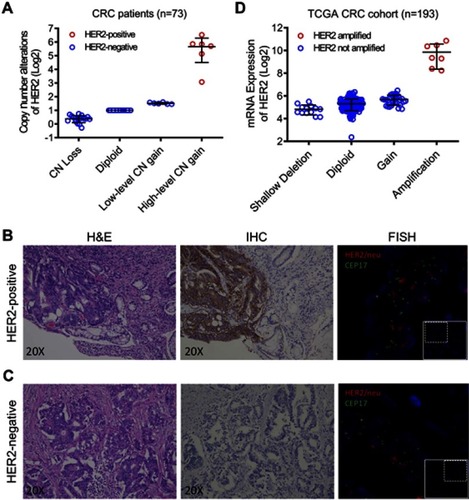
Figure 2 Genetic alterations of HER2-positive and -negative colorectal cancers (CRCs). (A) Mutation status of TP53, APC, KRAS, NRAS, BRAF, and PIK3CA in 6 HER2-positive and 67 HER2-negative CRCs. Lolliplots showing the distribution of KRAS (B) and PIK3CA (C) mutations in HER2-positive CRCs.
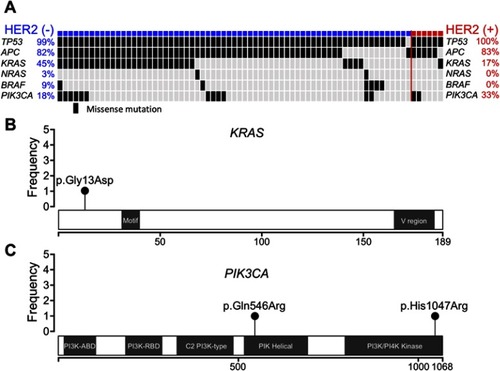
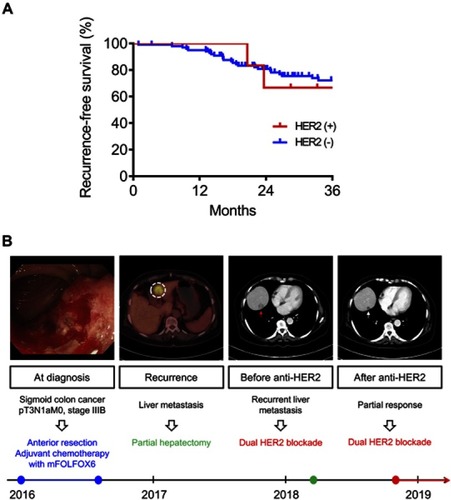
Figure 3 Clinical outcomes of HER2-positive and -negative colorectal cancers (CRCs). (A) Kaplan–Meier estimates of recurrence-free survival for HER2-positive and -negative patients with CRC. (B) A 75-year-old lady was diagnosed with stage III sigmoid colon cancer in the end of 2015. Standard surgical resection was performed at that time followed by adjuvant chemotherapy with mFOLFOX6. Liver metastases (white dotted circle) developed 2 years later. Despite curative surgical resection, recurrent liver metastases (red arrow) were detected soon after the surgery for liver metastases. Dual anti-HER2 blockade was initiated based on HER2 overexpression in both primary and recurrent tumors. Computed tomography scans obtained 2 months after anti-HER2 therapy demonstrated significant shrinkage of liver metastases (white arrow).