Figures & data
Figure 1 Overall study design. Firstly, all patients were divided into nodule group and mass group according to the size of the lesion; secondly, patients were divided into unidentified lesions group (before pathological confirmation) and lung cancer group (after pathological confirmation).
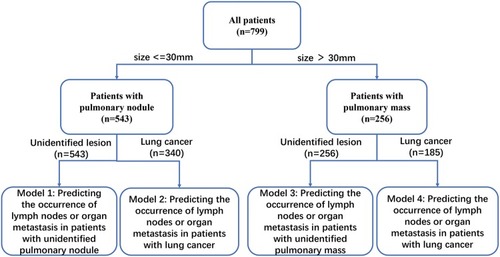
Table 1 Patient demographic and clinical data
Table 2 Serum level of tumor markers in different lesions
Table 3 The distribution of tumor markers based on the cut-off values
Table 4 The results of logistic regression based on different lesions
Figure 2 Development of nomogram to predict the occurrence of lymph node or organ metastasis in patients with nodules. (A) Model 1: for predicting the occurrence of lymph node or organ metastasis in patients with unidentified pulmonary nodule (size≤30 mm). To use the nomogram, an individual patient’s value is located on each variable axis, and a line is drawn upward to determine the number of points received for each variable value. The sum of these numbers is located on the Total Points axis, and a line is drawn downward to Risk axes to determine the risk of metastasis in patients with unidentified lesions. (B) The calibration curve for predicting the occurrence of lymph node or organ metastasis in patients with unidentified pulmonary nodules. (C) Decision curve analysis of nomograms based on model 1. (D) Model 2: for predicting the occurrence of lymph node or organ metastasis in patients with lung cancer (size≤30mm). (E) The calibration curve for predicting the occurrence of lymph node or organ metastasis in patients with lung cancer (size≤30mm). (F) Decision curve analysis of nomograms based on model 2.
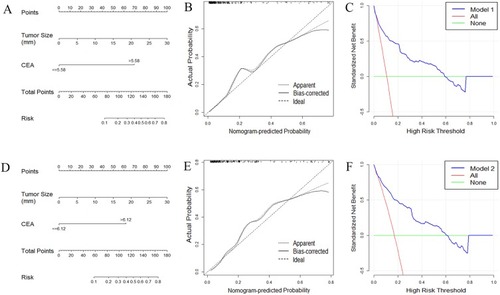
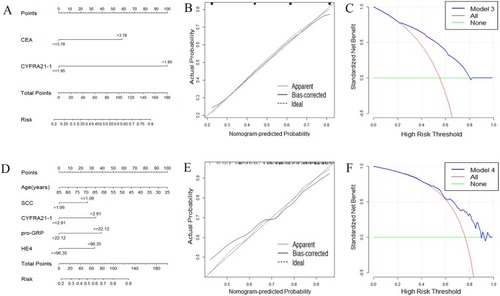
Figure 3 Development of nomogram to predict the occurrence of lymph node or organ metastasis in patients with mass. (A) Model 3: for predicting the occurrence of lymph node or organ metastasis in patients with unidentified pulmonary mass (size >30 mm). To use the nomogram, an individual patient’s value is located on each variable axis, and a line is drawn upward to determine the number of points received for each variable value. The sum of these numbers is located on the Total Points axis, and a line is drawn downward to Risk axes to determine the risk of metastasis in patients with unidentified lesions. (B) The calibration curve for predicting the occurrence of lymph node or organ metastasis in patients with unidentified pulmonary mass. (C) Decision curve analysis of nomograms based on model 3. (D) Model 4: for predicting the occurrence of lymph node or organ metastasis in patients with lung cancer (size >30mm). (E) The calibration curve for predicting the occurrence of lymph node or organ metastasis in patients with lung cancer (size >30 mm). (F) Decision curve analysis of nomograms based on model 4.