Figures & data
Figure 1 Examples of salvage therapy regimens for refractory NHL.
Notes:1Radiommunotherapy options include 131I-tositumomab and 90Y-ibritumomab tiuxetan; 2therapy for systemic ALCL, excluding primary cutaneous ALCL. Treatment options, stratification, and abbreviations are based on NCCN Clinical Practice Guidelines In Oncology (NCCN Guidelines®) for Non-Hodgkin’s Lymphomas V.1.2013. Not all treatment options included in the NCCN Guidelines are shown above. Reproduced/Adapted with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Non-Hodgkin’s Lymphomas V.1.2013. © 2013 National Comprehensive Cancer Network, Inc. All rights reserved. The NCCN Guidelines® and illustrations herein may not be reproduced in any form for any purpose without the express written permission of the NCCN. To view the most recent and complete version of the NCCN Guidelines, go online to NCCN.org. National Comprehensive Cancer Network®, NCCN®, NCCN Guidelines®, and all other NCCN Content are trademarks owned by the National Comprehensive Cancer Network, Inc.Citation131
Abbreviations: CEOP, cyclophosphamide, etoposide, vincristine, prednisone; CEPP, cyclophosphamide, etoposide, prednisone, procarbazine; CFAR, cyclophosphamide, fludarabine, alemtuzumab, rituximab; CHOP, cyclophosphamide, doxorubicin, vincristine, prednisone; CLL/SLL, chronic lymphocytic leukemia/small lymphocytic lymphoma; DA-EPOCH, dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin; DHAP, dexamethasone, cisplastine, cytarabine; DLBCL, diffuse large b-cell lymphoma; ESHAP, etoposide, methylprednisolone, cytarabine, cisplatin; FCR, fludarabine, cyclophosphamide, rituximab; FCMR, fludarabine, cyclophosphamide, mitoxantrone, rituximab; FL, follicular lymphoma; FMR, fludarabine, mitoxantrone, rituximab; GDP, gemcitabine, dexamethasone, cisplatin; GemOx, gemcitabine, oxaliplatin; HyperCVAD, fractionated cyclophosphamide, vincristine, doxorubicin, dexamethasone; ICE, ifosphamide, carboplatin, etoposide; MCL, mantle cell lymphoma; OFAR, oxaliplatin, fludarabine, cytarabine, rituximab; PCR, pentostatin, cyclophosphamide, rituximab; PTCL, peripheral T-cell lymphoma; R, rituximab; RFND, rituximab, fludarabine, mitoxantrone, dexamethasone; SCT, stem cell transplant.
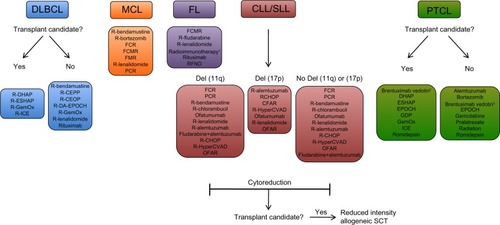
Figure 2 Emerging therapeutic options in relapsed/refractory NHL. Numerous novel classes of drugs are emerging as therapeutic options in relapsed or refractory NHL. These classes include monoclonal antibodies (both next-generation anti-CD20 and non-anti-CD20 antibodies), antibody–drug conjugates, antibodies conjugated to radioactive isotopes, small-molecule inhibitors of key cell-signaling and apoptotic pathways, HDAC inhibitors, and toxicity-reducing chemotherapies.
Abbreviations: abs, antibodies; Bcl-2, B-cell lymphoma 2; BTK, Bruton tyrosine kinase; HDAC, histone deacetylase; mTOR, mammalian target of rapamycin; NHL, non-Hodgkin’s lymphoma; Syk, spleen tyrosine kinase; PI3K, phosphoinositide 3-kinase.
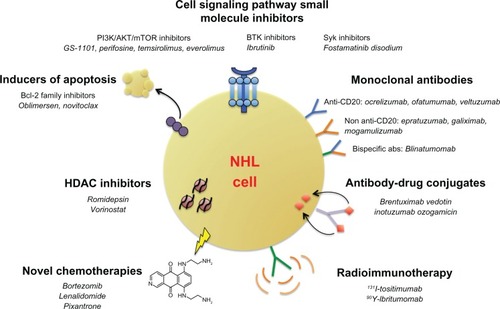
Table 1 Emerging antibody therapies in non-Hodgkin’s lymphoma
Figure 3 Targeting the PI3K and BTK pathways in NHL. The B-cell receptor-signaling pathway (purple) is initiated through phosphorylation of coreceptors that recruit spleen tyrosine kinase (SYK), which then phosphorylates downstream kinases, including PLCγ, leading to activation of Bruton tyrosine kinase (BTK). BTK then binds phosphatidylinositol (3,4,5)-triphosphate (PIP3), which in turn hydrolyzes phosphatidylinositol 4,5-bisphosphate (PIP2) into two second messengers – inositol triphosphate (IP3) and diacylglycerol (DAG) – that ultimately activate downstream proteins involved in B-cell signaling. In the PI3K pathway (orange), activation of receptor tyrosine kinases (RTKs) through adaptor proteins phosphorylate subunits of PI3K, leading to conversion of PIP2 to PIP3. Phosphorylation of the tumor suppressor PTEN terminates PI3K. Accumulation of PIP3 leads to phosphorylation of AKT, which further activates downstream pathways, including mTOR (through the tuberous sclerosis complex 1/2 (TSC1/2)) and other essential pathways. Therapeutic inhibition of select pathway components that have been investigated in clinical trials for NHL are shown.
Abbreviations: 4EBP-1, 4E-binding protein 1; GSK3, glycogen synthase kinase 3; mTOR, mammalian target of rapamycin; mTORC, mTOR complex; MDM2, mouse double minute 2 homolog; P, phosphorylation site; PI3K, phosphoinositide 3-kinase; PLC, phospholipase C gamma; PTEN, phosphatase and tensin homolog; RHEB, Ras homolog enriched in brain; S6K, S6 kinase.
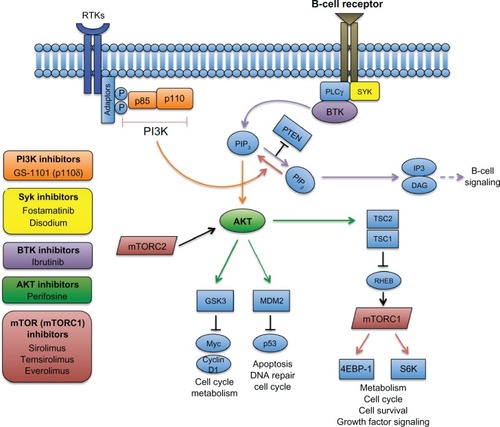
Table 2 Emerging non-antibody therapies in non-Hodgkin’s lymphoma