Figures & data
Figure 1 Treatment protocol.
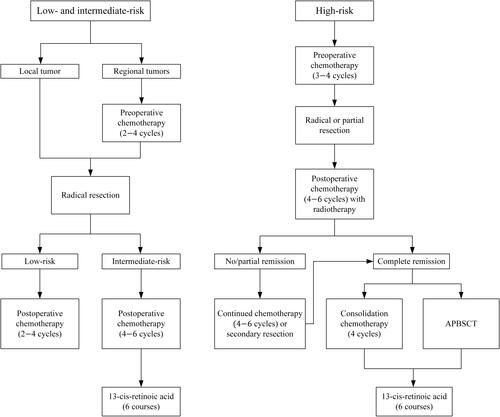
Table 1 Clinical Features of the Entire Cohort
Table 2 Overall Survival of Each Group in Children with Neuroblastoma After Initial Complete Response
Figure 2 (A) Overall survival (OS) of 179 children with complete response; (B) Comparison of OS between recurrence group and non-recurrence group; (C) Comparison of OS in different COG risk groups. (Kaplan–Meier method, P value shown for Log rank test among variables).
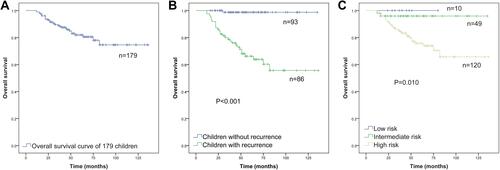
Table 3 Comparison of RFSs in 179 Children with Neuroblastoma After Initial Complete Response
Figure 3 (A) Recurrence-free survival (RFS) of 179 children with complete response; (B) Comparison of RFS in different COG risk groups. (Kaplan–Meier method, P value shown for Log rank test among variables).
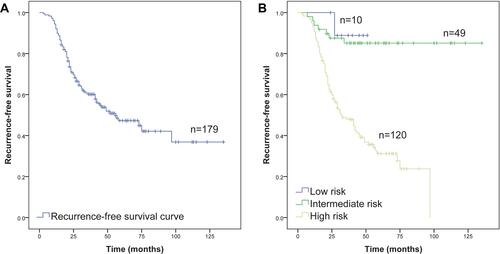
Figure 4 Comparisons of recurrence-free survival by (A) age, (B) gender, (C) INSS stage, (D) histological type, (E) primary site, and (F) bone marrow metastasis in 179 children with neuroblastoma. (Kaplan–Meier method, P value shown for Log rank test among variables).
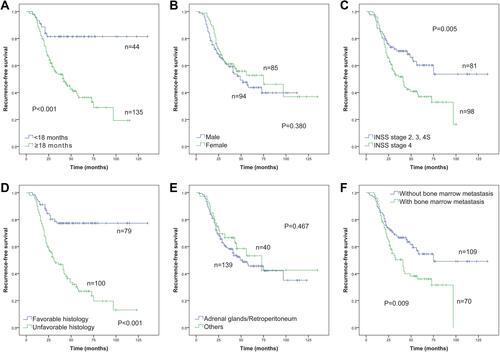
Figure 5 Comparisons of recurrence-free survival by (A) osseous metastasis, (B) hepatic metastasis, (C) distant lymph node metastasis, (D) MYCN status, (E) serum NSE level, and (F) serum LDH level in 179 children with neuroblastoma. (Kaplan–Meier method, P value shown for Log rank test among variables).
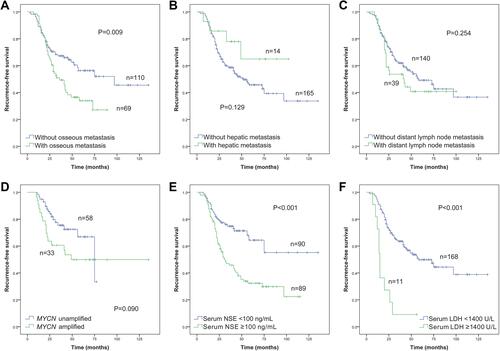
Table 4 Cox Proportional Hazard Model for the Unadjusted and Adjusted Risk Factors of Post-Remission Recurrence in 179 Children with Neuroblastoma
Table 5 Comparison of RFSs in 120 Children with High-Risk Neuroblastoma After Initial Complete Response
Figure 6 (A) Comparisons of recurrence-free survival by (A) age, (B) histological type, (C) hepatic metastasis, and (D) serum LDH level in 120 children with high-risk neuroblastoma. (Kaplan–Meier method, P value shown for Log rank test among variables).
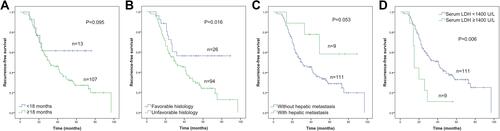
Table 6 Cox Proportional Hazard Model for the Unadjusted and Adjusted Risk Factors of Post-Remission Recurrence in 120 Children with High-Risk Neuroblastoma
Table 7 The New Recurrence Risk Stratification System and Previous Risk Classification Systems in Predicting Post-Remission Recurrence in Children with Neuroblastoma
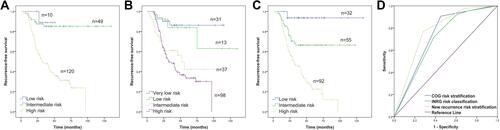
Figure 7 Recurrence-free survival of 179 children with neuroblastoma based on (A) COG risk stratification, (B) INRG classification system, and (C) the new recurrence risk stratification; (D) Comparison of ROC curves among the three stratification systems.