Figures & data
Figure 1 Midsagittal (left panel) and parasagittal (middle and right panel) T2 weighted MRI of brain in a 8 year old male child with AT/RT showing a bulky (5.3 cm × 3.1 cm), heterogeneous, intracranial mass in the posterior fossa involving the fourth ventricle, cerebellar vermis, midbrain and pineal region, pushing the brainstem anteriorly and cerebellum posteriorly; the tumor is lifting the tentorium cerebelli and causing herniation of the cerebellar tonsils in the middle panel; the tumor is abutting the straight sinus in the right panel; intra-tumor necrosis is better appreciated in middle and right panel.
Abbreviation: MRI, magnetic resonance imaging; AT/RT, atypical teratoid/rhabdoid tumor.
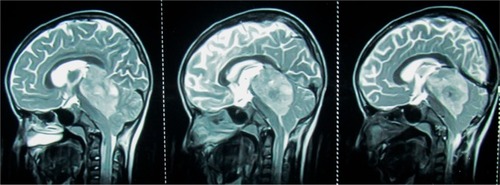
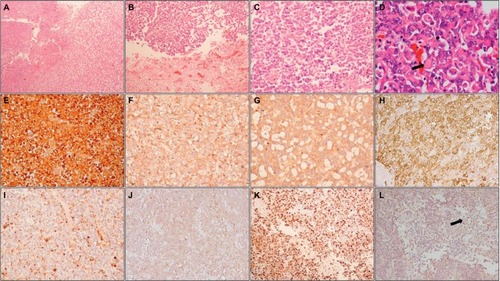
Figure 2 Histopathology and immunohistochemistry of AT/RT.
Notes: Photomicrographs showing a heterogeneous tumor (A; HE, 100×) with areas of necrosis (B; HE, 100×) composed of small round cells admixed with cells with eosinophilic cytoplasm (C; HE, 200×); higher magnification shows typical rhabdoid cells (arrow) (D; HE, 400×). On IHC, tumor cells are positive for vimentin (E; IHC, 200×), EMA (F; IHC, 200×), synaptophysin (G; IHC, 200×), SMA (H; IHC, 200×), and focally for GFAP (I; IHC, 200×) and cytokeratin (J; IHC, 200×); MIB-1-LI is high (K; IHC, 200×) and tumor cells show loss of INI1, while endothelial cells (arrow) show retained expression (L; IHC, 200×).
Abbreviations: HE, hematoxylin and eosin; IHC, immunohistochemistry; EMA, epithelial membrane antigen; SMA, smooth muscle actin; GFAP, glial fibrillary acidic protein; MIB-1-LI, MIB-1 labeling index; INI1, integrase interactor 1; AT/RT, atypical teratoid/rhabdoid tumor.