
Figures & data
Figure 1 Spanish population ≥ 40 years with diagnosed and treated COPD.
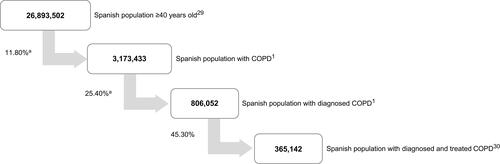
Figure 2 Distribution of patients considered in each GOLD group and GesEPOC phenotype in the base case analysis (A and B) and scenario analysis 1 (C), based on literature a. (A) Distribution of patients according to the GOLD strategy used in the base case analysis.Citation17 (B). Distribution of patients according to the GesEPOC guide used in the base case analysis.Citation17 (C). Distribution of patients to each GesEPOC phenotype used in scenario analysis 1.Citation9
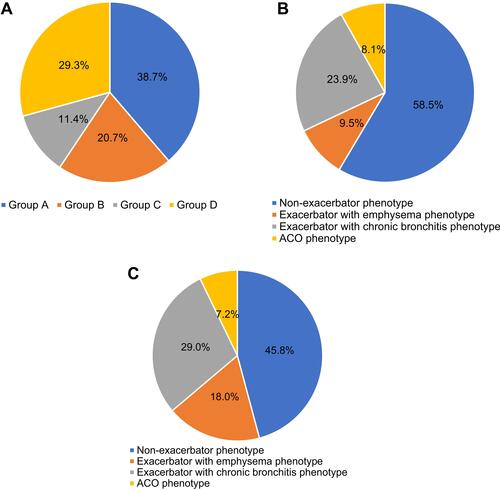
Figure 3 Base case analysis: current treatment patterns and proposed treatment according to GOLD (A) and GesEPOC (B) recommendations. (A) Current treatment patterns in pulmonology according to GOLD groupsCitation17 and proposed treatment patterns based on the GOLD strategy.Citation5 (B) Current treatment patterns in pulmonology according to GesEPOC phenotypesCitation17 and proposed treatment patterns based on the recommendations of the GesEPOC guidelines.Citation6
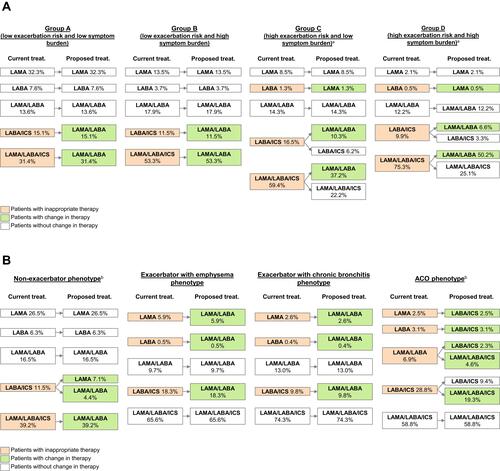
Table 1 Annual Pharmacological Cost Considered by Each Therapeutic Group
Table 2 COPD Patients Not Adherent to GOLD Recommendations and GesEPOC Guidelines in Pulmonology Units (Base Case Analysis)
Figure 4 Pharmaceutical expenditure and annual savings in patients treated in exclusively pulmonology services (base case analysis) (A and B) or pulmonology and primary care (scenario analysis 1) (C). (A) Following recommendations of the GOLD strategy (base case). (B) Following recommendations of the GesEPOC guide (base case). (C) Following the recommendations of the GesEPOC guide (scenario analysis 1).
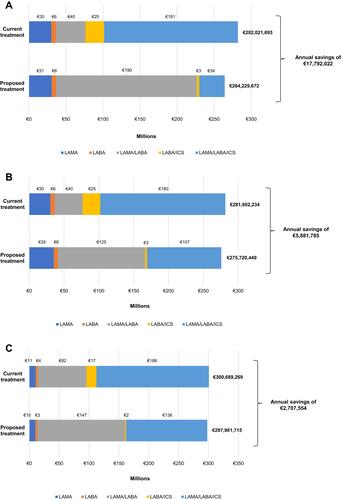
Figure 5 Base case analysis: annual savings in pharmaceutical expenditure in patients treated in pulmonology services distributed by Autonomous Community according to the GOLD (A) and GesEPOC (B) guidelinesa. (A) Following GOLD strategy recommendations. (B) Following GesEPOC guideline.
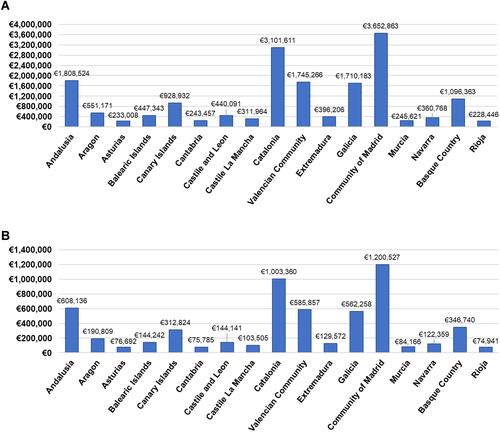
Table 3 COPD Patients Treated Without Following GesEPOC Guidelines in Pulmonology and Primary Care Units (Scenario Analysis 1)