Figures & data
Figure 1 Mechanisms underlying COPD development. Multiple risk factors including cigarette smoke and other irritants activate alveolar macrophages and epithelial cells in the respiratory tract leading oxidative stress followed release of multiple inflammatory mediators. These inflammatory mediators, particularly chemokines, attract neutrophils and monocytes as well as T helper cells. The activated alveolar macrophages and epithelial cells also release proteases such as neutrophil elastase and matrix metalloproteinase 9 (MMP-9), which damage the lung parenchyma resulting in lung vascular remodeling, alveolar wall destruction and mucus hypersecretion. In addition, the activated macrophages and epithelial cells release fibrogenic mediators, such as TGFβ which causes EMT and eventually small airway fibrosis.
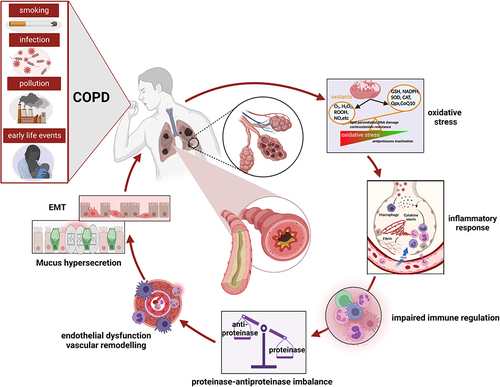
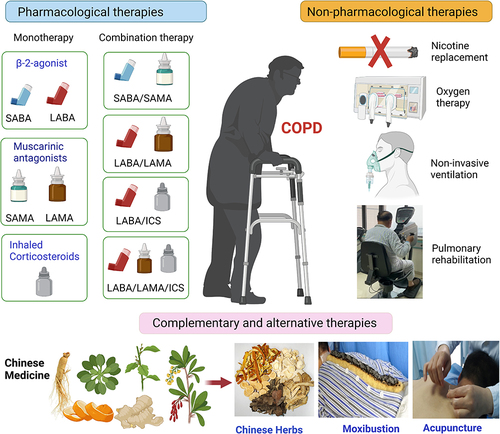
Figure 2 Schematic graph for conventional and complementary and alternative therapies treatment of COPD. Current pharmacological therapies for COPD contains short and long-acting β2-agonist, muscarinic antagonists and inhaled corticosteroids. Combination of two or three of them is commonly used in clinical practice. Nicotine replacement, oxygen therapy, pulmonary rehabilitation and non-invasive ventilation are main non-pharmacological therapies. There are complementary and alternative therapies, such as the use of PDE3/PDE4 inhibitors, RNA targeted drugs and Chinese medicine.