Figures & data
Figure 1 (A and B) Schematic illustration of how to calculate Ptf.
Notes: (A) Biphasic P-wave in V1. (B) Full negative P-wave in V1.
Abbreviation: s-Ptf, significant P-terminal force.
Abbreviation: s-Ptf, significant P-terminal force.
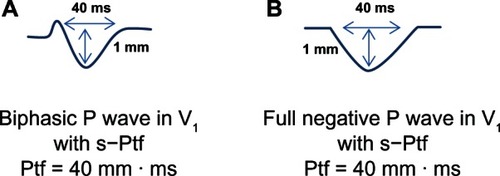
Table 1 Incidence of IAB, s-Ptf and type of P-wave morphology in lead V1 in emphysema patients based upon the presence of vertical or non-vertical P-vector
Figure 2 Schematic illustration of the incidence of interatrial block (IAB) and significant P-terminal force (s-Ptf) in emphysema patients.
Abbreviations: IAB, Interatrial block; s-Ptf (+), presence of significant P-terminal force; s-Ptf (−), absence of significant P-terminal force.
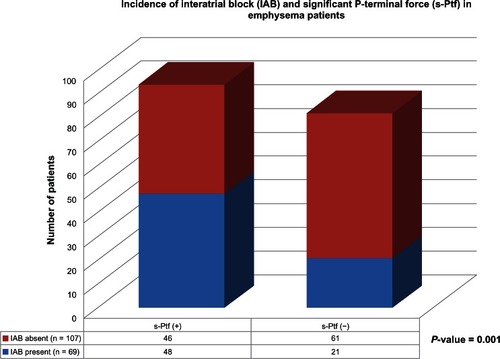
Figure 3 Distribution of types of P-terminal force (Biphasic vs. Fully negative) based on the presence or absence of interatrial block.
Abbreviations: IAB, interatrial block; s-Ptf, significant P-terminal force.
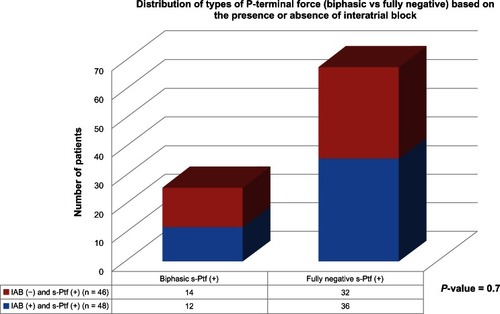
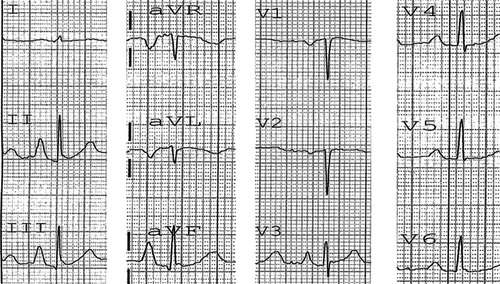
Figure 4 Electrocardiogram of a patient with emphysema.
Notes: Vertical P-vector and P pulmonale is present. Note the presence of a fully negative P-wave in V1 with significant P-terminal force (approximately 80 mm.ms). Based on the presence of P pulmonale and suspected right atrial strain/enlargement, one should expect a tall initial positive P-component in V1, which is in fact absent, suggesting primary contribution of diaphragmatic flattening and right atrial anatomical distortion to the generation of vertical P-vector.