Figures & data
Table 1 Pre-MS and MS subtypes as potential targets for oral therapies
Figure 1 Attempts to identify disease activity earlier than clinically definite relapsing-remitting MS (RRMS) has resulted in the identification of “McDonald Criteria” MS, clinically isolated syndrome (CIS), and radiologically isolated syndrome (RIS) based around MRI.
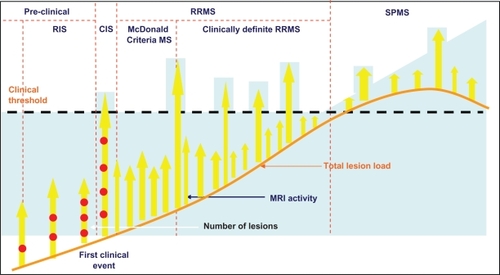
Figure 2 Resetting immune tolerance can prevent subsequent disability (A); however evidence is emerging that beyond a certain point during the course of MS, a “relapse-suppressive therapy” is not effective (B).
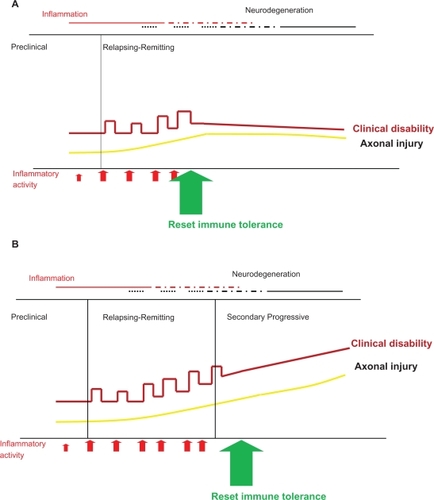
Figure 3 Annualized relapse rates observed in the 26 trials identified in the systematic review by Nicholas et alCitation21 plotted against the year in which the paper was published. The dashed line shows the fitted trend line.
Adapted from Nicholas et al.Citation21 Copyright © 2011, SAGE Publications. http://msj.sagepub.com
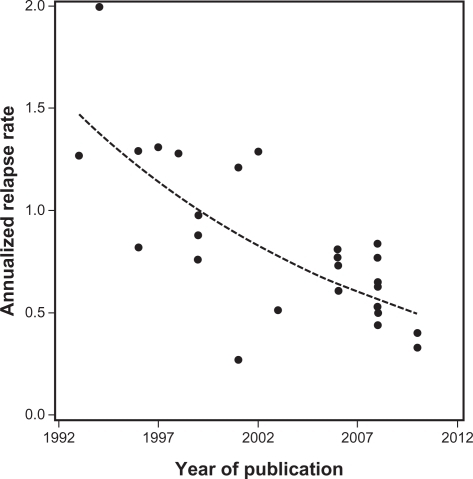
Table 2 Using data from placebo groups over 2 years based on 100 subjects in each group to predict the number of expected relapses
Figure 4 Simplified overview of postulated mechanism of action of standard injectables and new oral therapies. Fingolimod and cladribine reduce available circulating lymphocytes by blockade of lymphocyte egress from lymph nodes (fingolimod), by cytotoxicity and depletion (cladribine). Natalizumab acts by blockade of adhesion and transmigration across the blood–brain barrier. All three drugs (fingolimod, cladribine, and natalizumab), indirectly (fingolimod and cladribine) or directly (natalizumab), reduce the number of lymphocyte in the central nervous system (CNS). In contrast, IFN-β and glatiramer acetate (GA) shift the balance of lymphocytes and modulate cytokine secretion. The newer oral therapies, terifluonamide, laquinimod, and BG-12, do not reduce lymphocytes in the CNS and appear to act in a similar way to IFN-β and GA by modulating cytokines and lymphocyte activation. None of these injectable (IFN-β and GA) and oral (terifluonamide, laquinimod, and BG-12) drugs appear to significantly reduce the numbers of circulating lymphocytes, suggesting an immunomodulatory rather than an immunosuppressive profile.
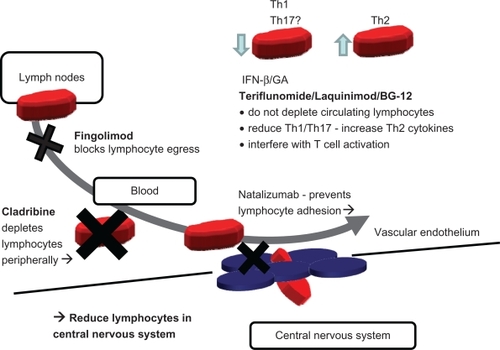
Table 3 Effect of therapy on long-term adherence