Figures & data
Figure 1 Model of TNSALP function in mineralizing cells.
Notes: Levels of the mineralization inhibitor, inorganic pyrophosphate (PPi), are controlled by activities of ectonucleotide pyrophosphatase phosphodiesterase 1 (ENPP1), the progressive ankylosis protein (ANKH/ANK), and tissue-non-specific alkaline phosphatase (TNSALP), all expressed by mineralizing cells. ENPP1 enzymatically cleaves nucleotide triphosphates (eg, adenosine triphosphate [ATP]) to generate PPi, while ANKH/ANK directs PPi transport to the extracellular space, both increasing pericellular PPi levels. TNSALP hydrolyzes PPi to allow inorganic phosphate (Pi) and calcium (Ca) to precipitate as hydroxyapatite (HAP), the inorganic component of bones and teeth. When TNSALP activity is lost in HPP, excess PPi inhibits HAP crystal initiation and growth, causing mineralization defects in the skeleton and dentition. Figure designed with images from Servier Medical Art (https://smart.servier.com/) under a Creative Commons Attribution 3.0 Unported License.
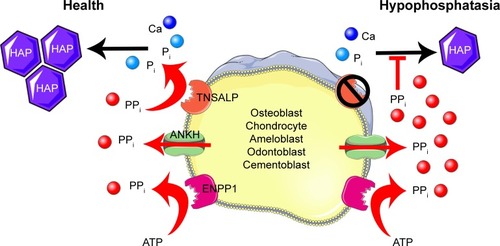
Figure 2 Skeletal and dental defects associated with hypophosphatasia.
Notes: (A) MRI of the skull of a 6-year-old individual with hypophosphatasia (HPP) exhibiting craniosynostosis and the resulting bregmatic bump. (B) Radiograph of a 4-year-old individual with HPP reveals hypomineralization of the cranial vault as seen by the “copper beaten” appearance of the skull. (C) Deformities of lower extremities with joint widening at knees and elbows in a 15-year-old boy with severe childhood HPP. (D) Knee radiograph of the same individual reveals hypomineralized bone, coarsened trabeculae, and an intramedullary rod in the tibia. A fracture line is seen at the diaphysis of the tibia (yellow arrow). (E) Goldner trichrome stain of normal iliac crest biopsy compared to (F) the same from an individual with adult HPP, showing accumulation of excessive osteoid (red layer indicated by black arrow) on the surface of the mineralized bone (green). (G) Oral photograph of a 2.5-year-old child with HPP exhibiting premature loss of primary lower incisors. (H) Primary incisors that spontaneously exfoliated from a child with HPP. Note the intact roots, a hallmark of HPP. (I) Oral radiograph of a 20-year-old individual diagnosed with odonto-HPP showing loss of secondary incisor, endodontic treatment after fracture, and splinting to try and stabilize remaining anterior teeth. Images in A and B are reprinted by permission from Springer Customer Service Centre GmbH: Springer Nature [Child’s Nervous System]; Neurosurgical aspects of childhood hypophosphatasia, Collmann H, Mornet E, Gattenlöhner S, Beck C, Girschick H. Copyright 2009.Citation31 Images in E and F are reprinted from Bone, Vol /edition 54(1), Berkseth KE, Tebben PJ, Drake MT, Hefferan TE, Jewison DE, Wermers RA, Clinical spectrum of hypophosphatasia diagnosed in adults, Pages 21–27, Copyright (2013), with permission from Elsevier.Citation36 Image in G is reproduced from Reibel A, Manière MC, Clauss F, et al. Orodental phenotype and genotype findings in all subtypes of hypophosphatasia. Orphanet J Rare Dis. 2009;4(1):6. Image in H is reproduced with permission from © 2017 American Society for Bone and Mineral Research. Whyte MP. Hypophosphatasia: enzyme replacement therapy brings new opportunities and new challenges. J Bone Miner Res. 2017;32(4):667–675.Citation112 Image in I is reproduced with permission from Copyright © 2012, John Wiley and Sons. Rodrigues TR, Georgetti AP, Martins L, Pereira Neto JS, Foster BL, Nociti Jr FH. Clinical correlate: case study of identical twins with cementum and periodontal defects resulting from odontohypophosphatasia. In: McCauley LK, Somerman MJ, eds. Mineralized Tissues in Oral and Craniofacial Science: Biological Principles and Clinical Correlates. 1st ed. Ames, IA: Wiley-Blackwell; 2012.Citation38
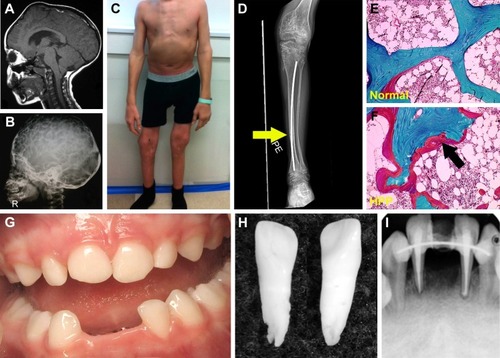
Figure 3 The Alpl−/− mouse model of severe infantile HPP.
Notes: (A) Radiographs of hind paws of wild-type (WT) and Alpl−/− mice at 22 days postnatal (dpn). Alpl−/− mouse phalanges and metatarsals (white arrows) show gross hypomineralization and deformities. (B) Radiographs of hind limbs of WT control and Alpl−/− mice at 22 dpn. Alpl−/− mouse femurs, tibias, and fibulas (white arrows) exhibit reduced mineralization, bowing, fracturing, and growth plate defects. (C) Radiographs of skulls of WT and Alpl−/− mice at 15 dpn. Alpl−/− mouse cranial bones feature severe hypomineralization and altered craniofacial shape. (D) Micro-computed tomography (micro-CT) of mandibles of WT and Alpl−/− mice at 14 dpn. Alpl−/− mouse molars, incisors, and alveolar bone show radiolucency indicative of severe hypomineralization. (E) Von Kossa-stained undecalcified tissue sections of WT and Alpl−/− mouse mandibles at 12 dpn. Compared to well mineralized molar dentin in WT (indicated by black stain), Alpl−/− mouse molar roots featured hypomineralized dentin matrix (lack of black stain). (F) H&E tissue sections of WT and Alpl−/− mouse mandibles at 22 dpn. Compared to the organized and functional periodontal complex in WT, Alpl−/− mouse molars exhibit lack (*) of acellular cementum (AC), detachment of the periodontal ligament (PDL), and disorganized PDL and alveolar bone. Images in panels A and B are reprinted from Bone, Vol /edition 49(2), Yadav MC, Lemire I, Leonard P, et al, Dose response of bone-targeted enzyme replacement for murine hypophosphatasia, Pages 250–256, Copyright (2011), with permission from Elsevier.Citation79 Images in panel C are reprinted from Bone, Vol 67, Liu J, Nam HK, Campbell C, Gasque KC, Millán JL, Hatch NE, Tissue-nonspecific alkaline phosphatase deficiency causes abnormal craniofacial bone development in the Alpl(−/−) mouse model of infantile hypophosphatasia, Pages 81–94, Copyright (2014), with permission from Elsevier.Citation71 Images in panel E are reproduced with permission from Copyright © 2013 American Society for Bone and Mineral Research. Foster BL, Nagatomo KJ, Tso HW, et al. Tooth root dentin mineralization defects in a mouse model of hypophosphatasia. J Bone Miner Res. 2013;28(2):271–282.Citation70
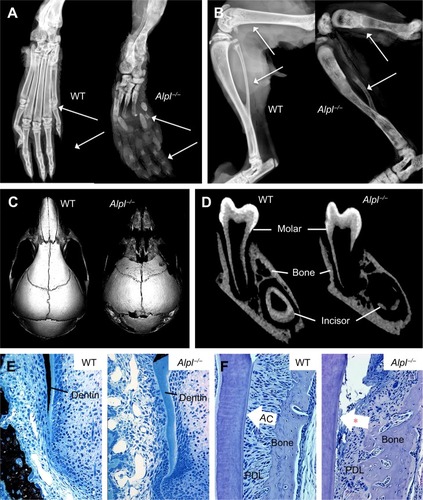
Figure 4 Asfotase alfa enzyme replacement therapy in a mouse model of HPP.
Notes: (A) Model of recombinant asfotase alfa enzyme showing tissue-non-specific alkaline phosphatase (TNSALP) dimer (blue), human IgG1 Fc domain (green), and D10 deca-aspartate tail (red). On the right, a simulated model shows predicted interaction of the highly negatively charged D10 tail with the positively charged calcium plane in hydroxyapatite (HAP) crystal. (B) Percent survival of wild-type (WT), untreated Alpl−/−, and Alpl−/− mice receiving 8.2 mg/kg asfotase alfa enzyme replacement therapy (ERT) over the course of the study. (C) Radiographs of hind limbs at 16 days postnatal (dpn) shows improvements in long bone lengths, shape, and appearance of secondary ossification centers in Alpl−/− mice receiving ERT. (D) Micro-computed tomography (micro-CT) of skulls at 15 dpn shows that ERT produces improvements in size, shape, and mineralization of craniofacial bones in Alpl−/− mice. (E) Von Kossa stained undecalcified tissue sections (left panels for each group) indicate that ERT rescues root dentin mineralization in Alpl−/− mice, as indicated by black stained appearance of mineralized tissues. H&E-stained sections (right panels for each group) reveal that ERT prevents acellular cementum (AC) hypoplasia (*) in Alpl−/− mouse molars, allowing periodontal ligament (PDL) attachment and normal periodontal architecture. Images in panel A are reproduced with permission (via republication of material within the agreed-upon thresholds between STM Permissions Guidelines signatories) from McKee et al.Citation81 Graph in panel B, images in panel C, and von Kossa images in panel E are reproduced with permission from Copyright © 2008 ASBMR. Millán JL, Narisawa S, Lemire I, et al. Enzyme replacement therapy for murine hypophosphatasia. J Bone Miner Res. 2008;23(6):777–787.Citation76 Images in panel D are reprinted with permission from Bone, Volume 78, Liu J, Campbell C, Nam HK, et al, Enzyme replacement for craniofacial skeletal defects and craniosynostosis in murine hypophosphatasia, Pages 203–211, Copyright (2015) with permission from Elsevier.Citation80 H&E images in panel E are previously unpublished data from BLF.
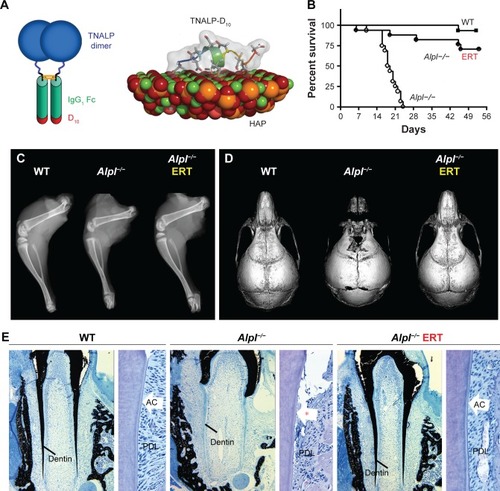
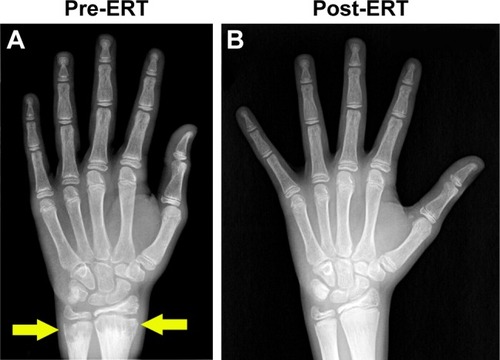
Figure 5 Asfotase alfa enzyme replacement therapy in human subjects.
Notes: Hand radiographs of a 15-year-old patient with severe childhood hypophosphatasia pre- and post-enzyme replacement therapy (ERT) treatment (6 months) with asfotase alfa. (A) Prior to ERT, marked metaphyseal fraying and characteristic “tongues” of radiolucency in the distal radius and ulna were evident (yellow arrow). (B) With asfotase alfa ERT, striking improvements in the previously abnormal radiolucency of the metaphyses was observed. Reprinted by permission from Springer Nature, Osteoporosis International, Asfotase alfa treatment for 1 year in a 16 year-old male with severe childhood hypophosphatasia, Bowden SA, Adler BH, Copyright 2018.Citation93