Figures & data
Table 1 Characteristics of the Study Population According to Baseline HbA1c Quartiles
Table 2 Association of the Liver Enzymes (Independent Variables) and Blood Glucose (Dependent Variable) According to Multiple Linear Regression Analysis
Table 3 Association of the Serum GGT and AKP Concentrations (Independent Variables) and Blood Glucose (Dependent Variable) According to Different Degrees of Fatty Liver and Liver Fibrosis
Table 4 Association of the Serum Liver Enzymes Concentrations (Independent Variables) and Blood Glucose (Dependent Variable) According to Binary Logistic Regression Analysis
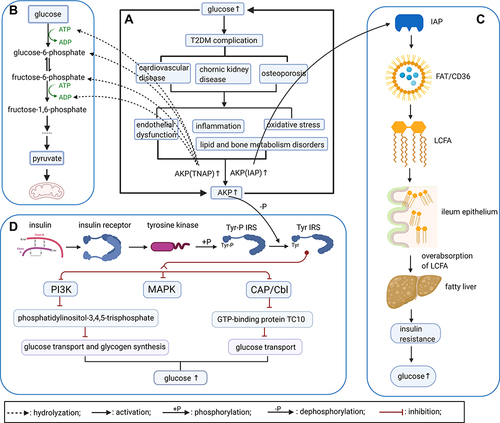
Figure 1 Interaction between elevated AKP concentrations and hyperglycemia (created with BioRender.com). (A) Persistent hyperglycemia will cause complications, such as cardiovascular disease, chronic kidney disease, osteoporosis, and pathological changes, including endothelial dysfunction, inflammation, oxidative stress and lipid and bone metabolism disorders, ultimately increasing AKP levels. (B) Normal aerobic oxidation and glycolysis in glucose metabolism. In the setting of hyperglycemia, increases in the AKP concentration can accelerate the hydrolysis of G-6-P, F-6-P, ATP, ADP, and other intermediate products of glucose metabolism, thereby accelerating the decomposition of glucose; this is a possible regulatory mechanism for elevating blood glucose level. (C) IAP and lipid metabolism. Dephosphorylation of the FAT/CD36 complex can promote LCFA entering the small intestine epithelial cells, thereby promoting fat absorption and metabolism, and IAP can accelerate this dephosphorylating process, leading to the overabsorption of fat, disorders of lipid metabolism and even promotion of fatty liver, and resulting in further aggravating the patient’s IR. Eventually, the blood glucose concentration cannot be adjusted to a normal level. (D) Through normal insulin signaling pathway, AKP may dephosphorylate the Tyr-phosphorylated insulin receptor substrates, leading to the failure of normal activation of PI3K and CAP/Cbl signalling pathways, thus inhibiting glucose transport and glycogen synthesis, causing the increase of blood glucose level.