Figures & data
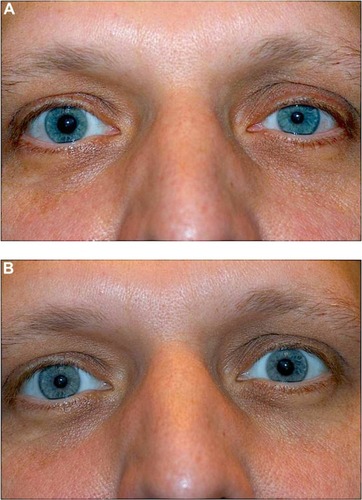
Figure 1 Right Horner syndrome in a 65-year-old man. Note right-sided upper lid ptosis, right miosis, and “upside-down” ptosis (ie, elevation) of right lower lid.

Figure 2 Drawing showing the anatomy of the oculosympathetic pathway.
Abbreviations: a, artery; n, nerve.
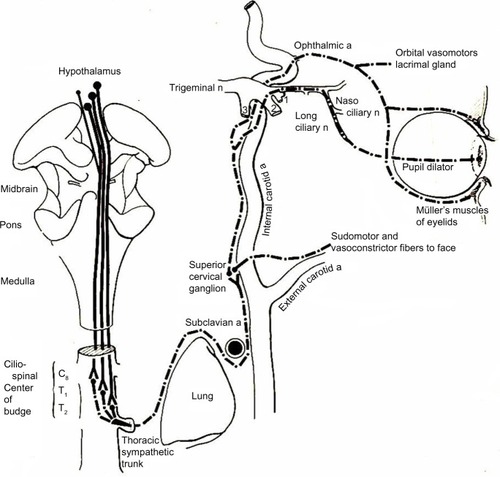
Figure 3 (A) Cadaver dissection showing oculosympathetic fibers (S) attaching (lower arrow) to the abducens nerve (VI) within the cavernous sinus. After running with the nerve for a short distance, they separate from the nerve (upper arrow) and join with the first division of the trigeminal nerve (V1) to enter the orbit.
Abbreviations: ON, optic nerve; ICA, internal carotid artery.
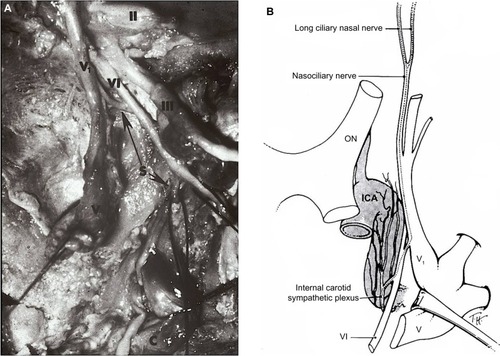
Figure 4 Infant with right Horner syndrome, demonstrating ipsilateral upper lid ptosis, “upside-down” ptosis of the lower lid, and anisocoria, with the right pupil smaller than the left. Both pupils reacted briskly to light stimulation.

Figure 5 Cocaine Testing for Horner Syndrome.
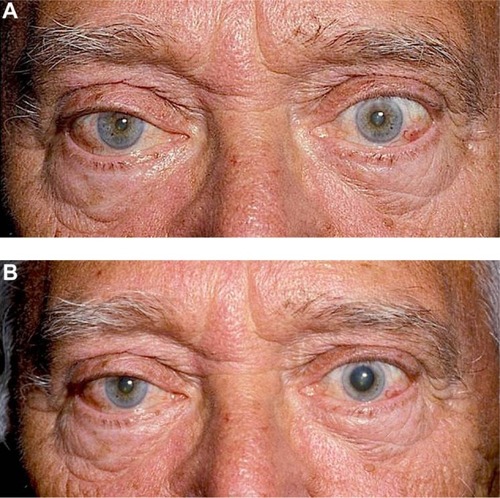
Figure 6 Apraclonidine Testing for Horner Syndrome.