
Figures & data
Figure 1 Fundus photograph of the left eye of a patient with HSV1-associated acute retinal necrosis shows marked optic disc edema associated with peripheral areas of retinal necrosis and retinal hemorrhages.

Figure 2 (A) Fundus photograph of the right eye of a patient with cat scratch disease showing optic disc edema and a complete macular star consistent with a diagnosis of neuroretinitis. (B) Late-phase fluorescein angiogram shows optic disc leakage with no abnormalities in the macular area. (C) Optical coherence tomography shows peripapillary serous retinal detachment.
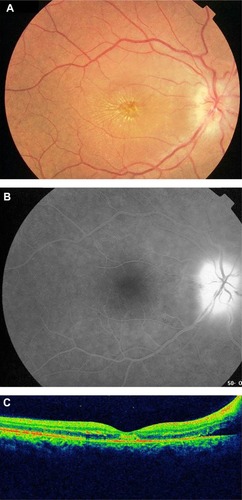
Figure 3 (A) Fundus photograph of the left eye of a patient with ocular tuberculosis shows a juxtapapillary choroidal granuloma with associated papillitis. Note the exudative retinal detachment surrounding the choroidal granuloma and the macular exudates. (B) Late-phase fluorescein angiogram shows leakage of the optic disc and granuloma.
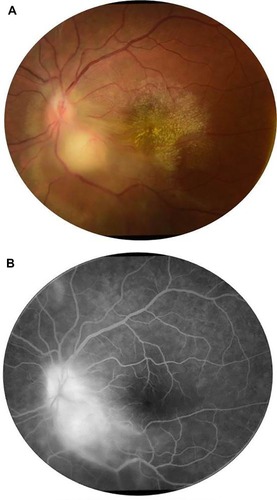
Figure 4 Fundus photograph of the left eye of a patient with rickettsial disease shows optic disc edema and a macular star. Note the presence of foci of inner retinitis in the superior periphery (arrows).
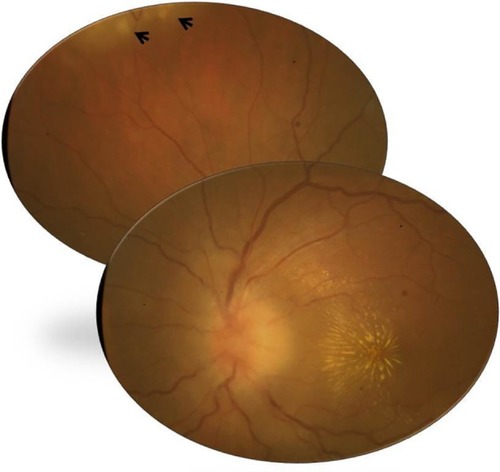
Figure 5 Fundus photograph of the left eye of a patient with a history of rickettsial infection shows optic disc atrophy secondary to ischemic optic neuropathy.
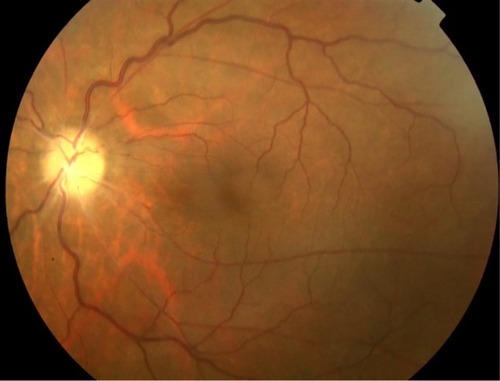
Figure 6 (A) Fundus photograph of the left eye of a patient with ocular toxoplasmosis shows a juxtapapillary active area of retinochoroiditis adjacent to a pigmented scar with associated serous retinal detachment. (B) Early-phase fluorescein angiogram shows hypofluorescence of both active and old foci. (C) Late-phase fluorescein angiogram shows peripheral hyperfluorescence and persistent central hypofluorescence of the active focus of retinochoroiditis with late pooling of dye in the subretinal space and optic disc hyperfluorescence. (D) Fundus photograph 6 months later shows a small atrophic retinochoroidal scar that replaced the active toxoplasmic lesion with a localized defect of the retinal nerve fiber layer as wedge-shaped area running toward the optic disc. (E) Goldmann perimetry shows a persistent scotoma.
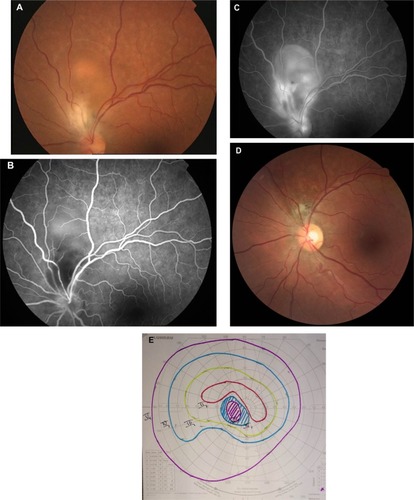
Figure 7 Practical approach to infectious optic neuropathies according to epidemiologic data and associated systemic involvement.
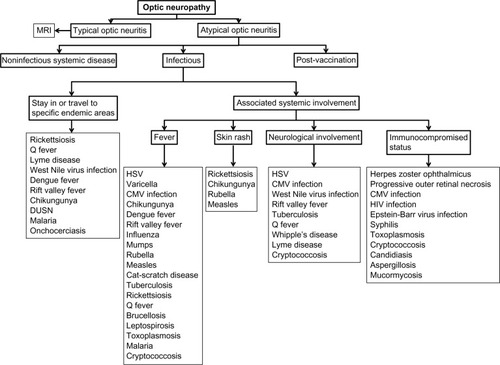
Figure 8 Practical approach to infectious optic neuropathies according to associated ocular findings.
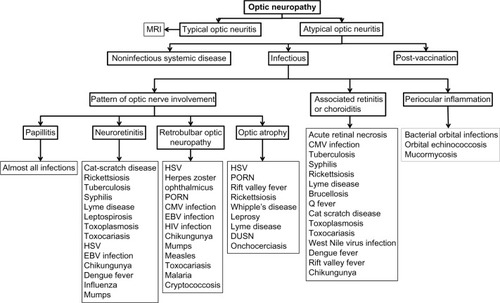
Table 1 Summary of findings in main infectious optic neuropathies