Figures & data
Figure 1 (A) Initial chest radiograph showing extensive airspace consolidation in the left lower lobe (black arrows) and numerous fine nodular opacities in both lungs (white arrows). There is no pleural effusion. Note a diffuse increase in bone density associated with the underlying MF. (B) Follow-up chest radiograph showing marked progression of bilateral pulmonary abnormalities and development of left pleural effusion (e). Note an enlarged splenic shadow (asterisk in (A) causing medial displacement of the gas-filled stomach. (C–D) Subsequent axial chest CT scans with lung-window (C) and mediastinal-window (D) settings showing multifocal consolidations (arrows) in bilateral upper and lower lobes with modest-sized left pleural effusion (e). Also, note an enlarged subcarinal lymph node with heterogeneous contrast enhancement (arrowhead in (C).
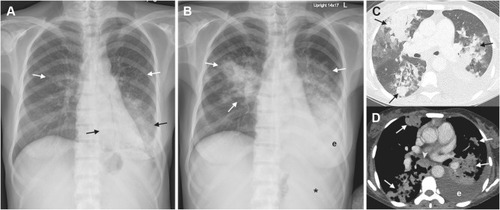
Figure 2 (A–C) Mucicarmine staining of BAL fluid cytology ((A), x400) show intracellular yeasts, engulfed by macrophages (arrow in (A)), and extracellular yeasts with thick capsule (arrowhead in (A). Histopathologic sections of the left lower lobe and right upper lobe biopsies reveal non-necrotizing granulomatous inflammation ((B), H&E stain, 400x) and organizing pneumonia ((C), H&E stain, 400x), respectively.
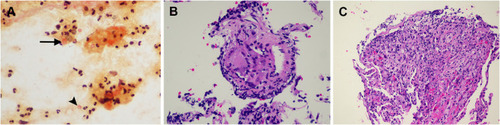
Figure 3 The follow-up chest radiography obtained after six months of antifungal therapy showing a marked decrease in the size of alveolar opacity at the right upper lung and left lower lung, including left pleural effusion.