Figures & data
Figure 1 Chest CT (A–F). (A and B) Diffuse nodules in the lungs and multiple paratracheal lymph node enlargements on January 1, 2018. (C and D) The diffuse nodular shadows in the lungs were significantly increased, multiple lymph nodes around the trachea were enlarged and were unchanged compared with those in (A and B), and a small amount of pleural effusion was observed on January 15, 2018. (E and F) The diffuse nodules in the lungs were decreased in size, and multiple lymph nodes around the trachea had decreased in size on February 5, 2018. (red and yellow arrows indicate two enlarged lymph nodes).
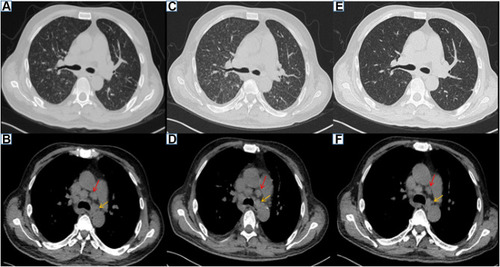
Figure 2 Bone marrow biopsy. (A–C) A small number of naive plasma cells were present away from the trabecular bone (no significant atypia), along with local fibrous hyperplasia with plasma cell hyperplasia (approximately 20%). (A) HE, ×400. (B) Masson staining (mild fibrous hyperplasia), ×400. (C) MPO (+), ×200.
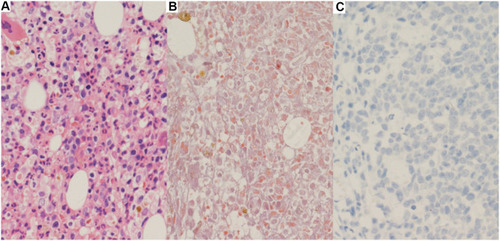
Figure 3 NSHL-related pathological results (A–D). (A) A background of complex inflammatory cells scattered with heterogeneous Hodgkin-like large cells. (B) CD30(+). (C) CD3(-). (D) PAX5(±) (all magnification times are x400).
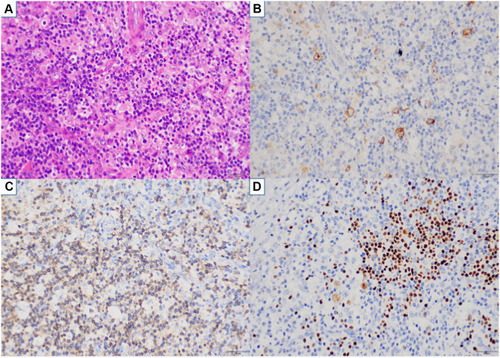
Figure 4 Bronchoscopic examinations. (A–C) The trachea and the walls of the left and right main bronchi are scattered with small nodules. The nodules are partially fused near the carina (the red arrow indicates the lesion site).
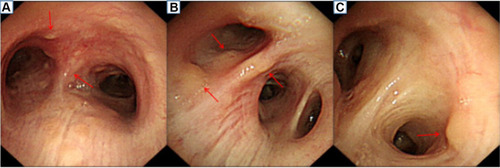
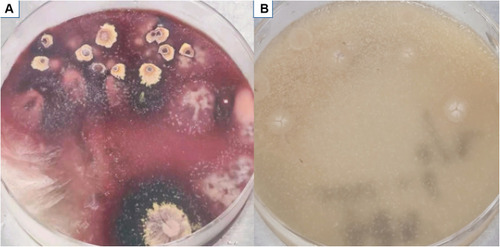
Figure 5 Microbiological examination-colony morphology (A and B). (A) T. marneffei presented in the mycelial phase, with the presence of broom branches and production of red pigment at 25°C. (B) Yeast phase at 37°C.