Figures & data
Figure 1 (A and B) X-ray demonstrated that the left femoral head exhibited a strip-like low-density area (yellow arrow) but no evidence of stenosis. (C) CT revealed the left femoral head remains regular, the continuity of the upper bone cortex is poor, patchy low-density areas (red arrow) can be seen under the articular surface, edge hardening, and slightly high-density foci can be seen considering the formation of dead bone. (D and E) MRI revealed necrosis of the left femoral head, and effusion in the left joint cavity (blue arrow). (F) No obvious abnormality in Hip X-ray half a year after discharge.
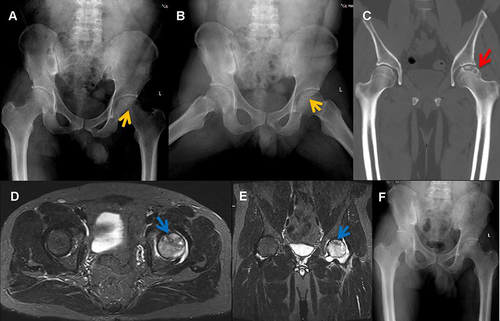
Figure 2 (A) Core biopsy of the right femoral head revealed necrotic material stained with HE. (B) Giemsa staining demonstrated scattered positive Brucella (red circle).
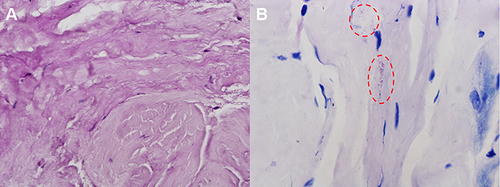
Figure 3 (A) X-ray of the Hip joint showed low signal on the right femoral head (yellow arrow), joint narrowing and even invagination of the joint space. (B) CT showed cavities necrosis and low-density patches of shadows (red arrow) in the right femoral head. (C) MRI showed effusion of the right Hip joint and necrosis of the right femoral head (blue arrow), and the inflammatory fluid diffused with extra-articular. (D–F) X-ray, CT and MRI of the osteonecrosis area four years later are better.
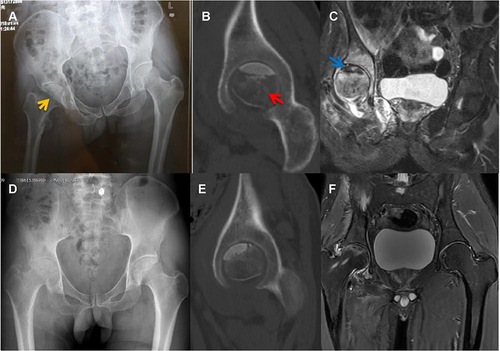
Figure 4 (A) HE staining showed partial dead bone and inflammatory cellulose exudate in osteonecrosis of the femoral head. (B) Giemsa staining revealed scattered positive Brucella (red circle).

Table 1 The Clinical Characteristics of Three Patients
Figure 5 (A and B) Right femoral head collapsed significantly (yellow arrow), joint space narrowed, and multiple areas of low density were seen (yellow arrow) on X-ray; in the left femoral head, the shape and joint space were normal, and low-density areas (yellow arrow) were visible. (C) CT showed hyperplasia and sclerosis of the bilateral acetabular margins, uneven bone density in the left femoral head (red arrow), and a huge cavity in the right femoral head (red arrow). (D) MRI showed extra-articular inflammatory fluid, bilateral Hip joint effusion and bilateral osteonecrosis of the femoral head (blue arrow), especially on the right side. (E) Right total hip arthroplasty was performed when the inflammatory indexes normalized. (F and G) X-ray showed the left femoral head collapsed and joint space narrowed (yellow arrow). (H) No abnormalities in Hip X-ray at the follow-up in January 2022.
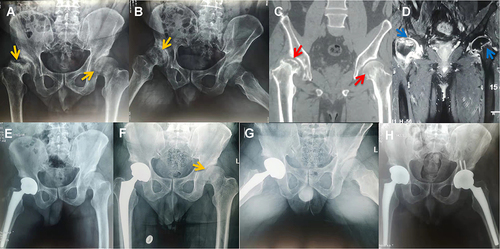
Table 2 Literature Review of Femoral Head Necrosis Due to Brucella Infection
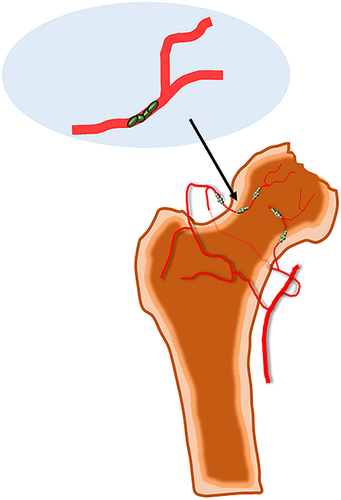
Figure 6 Rare bacterial avascular necrosis of the femoral head caused by Brucella infection, its pathogenesis may include bacterial invasion, vascular blockage and destruction of synovial tissue.