Figures & data
Table 1 Clinical and Laboratory Indicators of the Patient
Figure 1 Imaging examination. (A) Magnetic resonance imaging (MRI) of vertebra lumbalis showed a 26 mm × 73 mm subcutaneous abscess with low signal intensity on T1WI and high signal intensity on T2WI (arrows). (B) The chest radiograph showed that the patient’s lungs were normal.
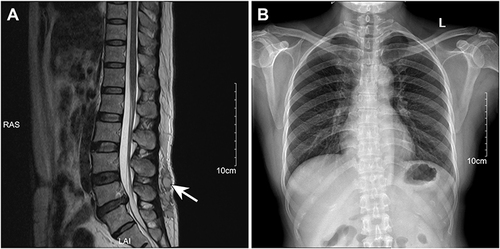
Table 2 Antimicrobial Susceptibility of the Nocardia Cyriacigeorgica by Kirby–Bauer method and Epsilometer Test
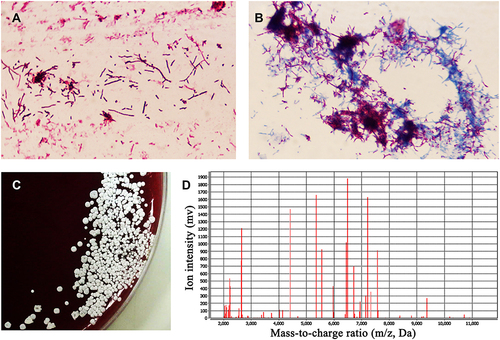
Figure 2 Pathogenic examination. (A) Gram-positive and branching rod-shaped bacterium was observed by Gram staining under oil mirror (×1000 magnification). (B) Acid fast staining showed weak positive mycelia, which proved that it was probably Nocardia spp. (C) Wrinkled, dry and white colonies of different sizes were observed by culture on the blood plate. (D) Matrix-assisted laser desorption ionization-time-of-flight mass spectrometry (MALDI-TOF MS) confirm it was Nocardia cyriacigeorgica.