
Figures & data
Table 1 Patient Laboratory Test Results
Figure 1 Exclusion of the proliferative neoplasms and indication the existence of infection by biopsy. (A) Body rashes were observed during physical examination on admission. Multiple rufous body rashes with central umbilication were scattered in the thoracoabdominal skin of the patient. (B) Nucleated cells in bone marrow smears showed normal blood picture of the patients with marked hyperplasia of active proliferation of erythroid, myeloid and megakaryocytes. (C and D) Histologic section of the mucosae from the pulmonary solid mass in the right upper lobe showed chronic active inflammation with organic consolidation. (E and F) Histologic section of the pulmonary solid mass in the right upper lobe showed multifocal areas of consolidation with fibrous polypoid tissue, alveolar epithelium and vascular hyperplasia in the alveolar cavity. A large number of lymphocytes, plasma cells, phagocytes and neutrophils were infiltrated in the lung tissue, and the pulmonary septum was widened, which suggested that chronic active inflammation of lung tissue with parenchymal lesions and bronchiolitis obliterans with organized pneumonia (BOOP). (B–F) The red arrow indicates the inflammatory infiltration area.
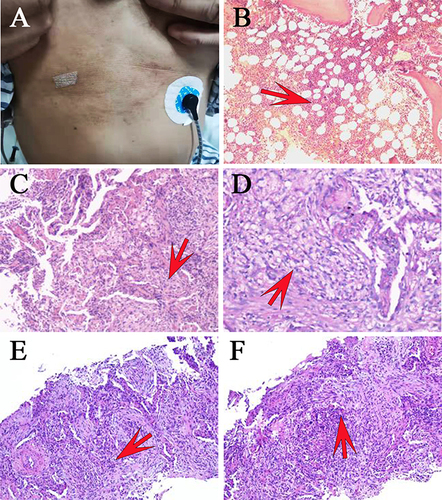
Figure 2 Monitoring of laboratory testing indicators during patient hospitalization. (A) Monitoring of hematological variables during the patient’s hospitalization. (B) Monitoring of infection markers during the patient’s hospitalization. (C) Monitoring of coagulation function indicators during the patient’s hospitalization. (D) Monitoring of biochemical indicators during the patient’s hospitalization.
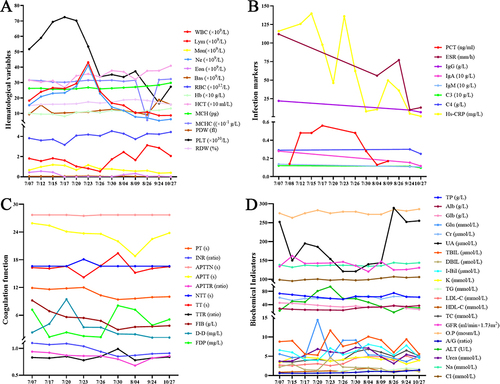
Figure 3 Patient medication status and outcomes. (A) Chest computed tomography (CT) showed an irregular solid nodule in the right upper lobe with apical bronchial occlusion, patchy infiltration and irregular thickening of local interlobular septum, fibrous foci and tiny nodules are seen in the left lower lobe, presenting with a right pleural effusion on July 8th 2021. CT images showed prominent improvement of pulmonary lesion with depauperation of patchy infiltration in original bilateral lung fields after effective antifungal therapy by voriconazole on Aug 4th 2021. CT reexamination showed that patchy high-density shadows of the two lungs were further absorbed on Aug 26th 2021. (B) Antibiotic anti-infective therapy timeline of the patient. (C) Body thermogram during treatment.
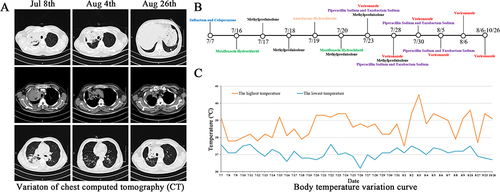
Figure 4 Etiological inspection and PCR amplification of the ITS region demonstrated talaromycosis and validated the variant. (A) PCR amplification for internal transcribed spacer (ITS) region in genomic DNA of the clinical isolate. Lane M: DNA ladder (Tsingke, China). Lane 1: negative control. Lane 2: amplicon (563 bp) of the strain with the ITS primers. (B) Acid-fast staining of sputum was negative in a suppurative inflammatory background with plentiful macrophages and neutrophils, which preliminarily excluded the Mycobacterial infection. (C) Blue fluorescent fungal spores were observed in the dark field indicating fungal infection by fungal fluorescence staining of sputum. (D) Gram staining of alveolar lavage fluid showed that deeply stained fungal spores were detected. The black arrow indicates a suspected discovery of fungal spores. (E) Microscopy analysis of the colonies grown on PDA at 28°C by lactophenol cotton blue staining. Scattered, slightly asymmetric and typical double-helical broom-like fungal hyphae with short, smooth walled, ellipsoidal, monoverticillate Penicillium conidiophores were observed (magnification × 1000). (F) Fungal culture of BALF revealed colonies with thermally dimorphic growth character, which showed yeast-like fungi producing soluble red pigment at 28 °C and mycelia at 37 °C in Candida nutrient agar (CANA), potato dextrose agar (PDA) and Sabouraud dextrose agar (SDA).
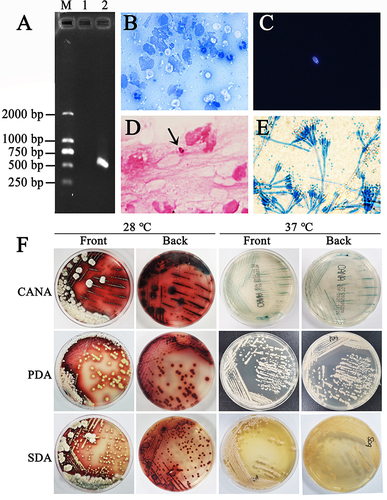
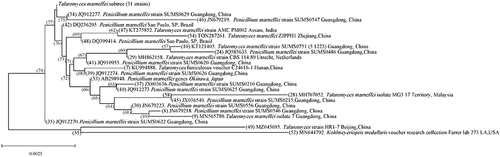
Figure 5 Phylogram of the clinical T. marneffei strain. It was based on ITS sequences and constructed utilizing the sequence of Talaromyces marneffei ZJPPH1 from the isolate of this study along with 53 available sequences with the highest homology retrieved from GenBank by MEGA11.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author Yumei Ge on reasonable request.