
Figures & data
Table 1 Cerebrospinal Fluid Results of Patient 1
Figure 1 MR findings on May 26: Multiple nodular lesions were observed in the bilateral cerebral, cerebellar, and basal ganglia regions, accompanied by peri-lesion edema and mild ring enhancement.
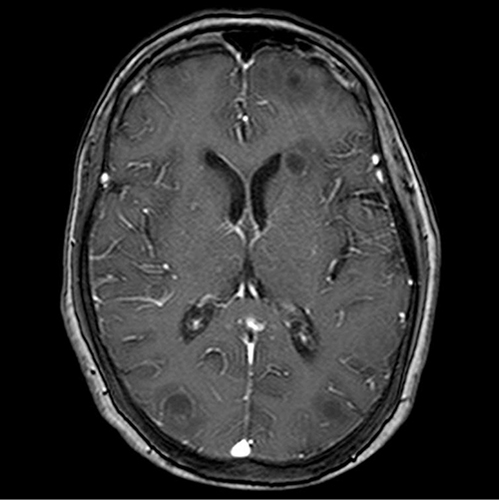
Figure 2 MR enhancement on June 6: Multiple ring-enhancing lesions were observed in bilateral cerebral and cerebellar hemispheres, along with perifocal edema and a uniform and smooth lesion ring wall. Pseudocontinuous arterial spin labeling (pCASL) and dynamic susceptibility contrast-enhanced perfusion-weighted imaging (DSC-PWI) demonstrated that the ring-enhancing lesions (solid portion) were hypoperfused, whereas diffusion-weighted imaging (DWI) demonstrated that diffusion was not obviously restricted, with most of the necrotic and liquefied areas within the lesion being significantly restricted in diffusion. Magnetic resonance spectroscopy (MRS) revealed a prominent lip peak in the lesion, along with diminished NAA, Cr, and Cho peaks, particularly the NAA and Cr peaks. (A) DWI sequence shows multiple nodular lesions in bilateral cerebral hemispheres, with low signal in the center of the lesion and high signal around it. (B) T2 sequence shows multiple nodular lesions in bilateral cerebral hemispheres with peripheral edema. (C) ADC sequence showed multiple nodular lesions in bilateral cerebral hemispheres, with high signal in the center of the lesion and low signal around it. (D) T2 sequence shows multiple nodular lesions in both cerebral hemispheres. (E) T1 enhanced scans showed multiple nodular lesions in both cerebral hemispheres, with ring-enhancement. (F) Multiple nodular high signal lesions in bilateral cerebral hemispheres of DWI sequence. (G) The ADC shows multiple nodular lesions in both cerebral hemispheres with low signal and restricted diffusion.
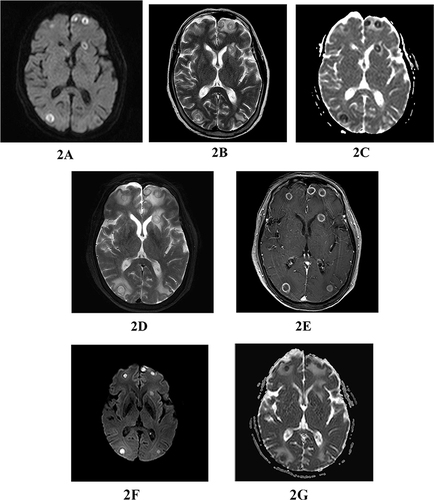
Figure 3 MR on June 29: multiple ring-enhancing lesions were still found in the bilateral cerebral and cerebellar hemispheres, which had shrunk significantly. (A) T1 enhancement sequence showed multiple circular enhancement lesions on both sides of the brain, marked perifocal edema, uniform, smooth ring wall, and ring-enhancement. (B) The T2 sequence shows that the lesion has a high signal, with significant surrounding edema.
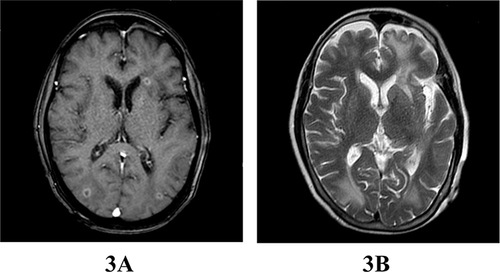
Table 2 Cerebrospinal Fluid Results of Patient 2
Figure 4 Cranial MR enhancement on July 28: There was meningeal thickening and abnormal enhancement, along with empyema adjacent to the cerebral falx and tentorium cerebelli. (A) T2 sequence showing a high signal bar on the left side of the cerebral falx, locally wrapped and considered to be empyema. (B) FLAIR sequence showing a low signal bar on the left side of the cerebral falx, locally wrapped.
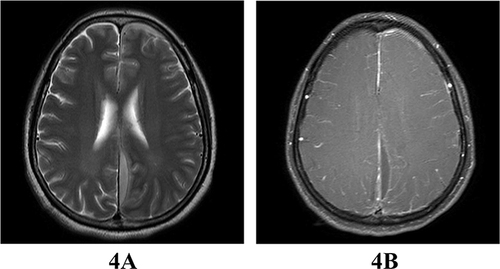
Figure 5 Cranial MR enhancement on August 13: Multiple abnormal signals were observed in the left frontoparietal lobe, the corpus callosum splenium, and the left temporal pole, along with thickening and abnormal enhancement of the meninges and empyema adjacent to the cerebral falx and tentorium cerebelli. (A) DWI sequence showing abnormally high signal in the left lateral semicircle of the cerebral falx, locally wrapped, with high signal on DWI. (B) Enhanced scan showing abnormally high signal in the left lateral semicircle of the cerebral falx, local encapsulation, local meningeal thickening, abnormal strengthening, and considered considered to be empyema. (C) ADC sequence showing abnormally high signal in the left side semicircle of the sickle, local encapsulation, hypoperfusion, and limited diffusion. (D) T2 sequence showing abnormally high signal in the left side semicircle of the falx of the brain, localized wrapping, and surrounding swelling.
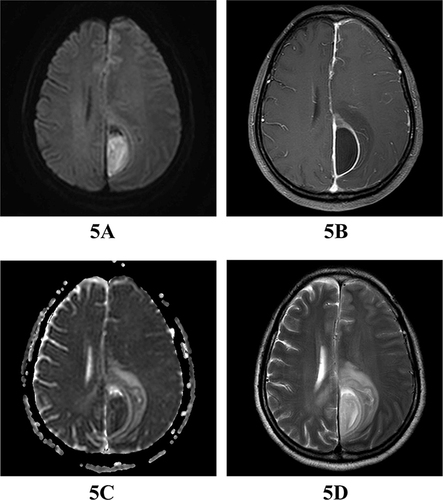
Figure 6 Cranial MR enhancement on August 24: Spindle-shaped ring enhancement was observed in the region adjacent to the left cerebral falx, the left tentorium cerebelli, and the adjacent brain parenchyma, where abnormal signals were still present. Compared to the previous MR, the range of enhancement and peripheral brain edema were reduced. (A) The T2 sequence shows a crescent-shaped high signal adjacent to the left side of the falx cerebri, with local encapsulation and surrounding edema. (B) T1 enhanced scan shows low signal intensity in the left hemisphere of the cerebral falx, local swelling, and ring-enhancement.
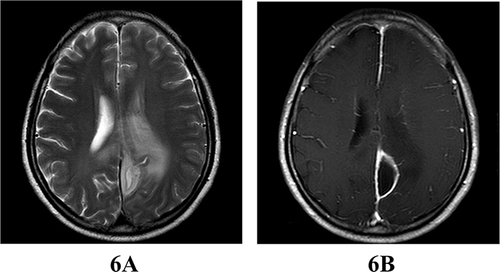
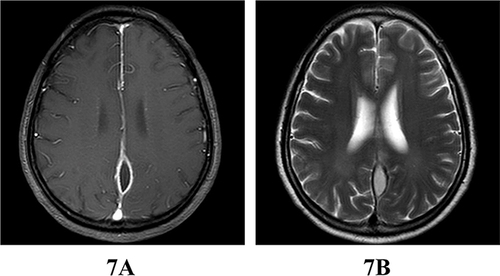
Figure 7 Cranial MR enhancement on September 23: Spindle-shaped ring enhancement was still visible in the region adjacent to the left cerebral falx and the left tentorium cerebelli, where abnormal signals were detected. In comparison to the previous MR, the extent of enhancement was diminished, and the original peripheral brain edema had dissipated. (A) The T1-enhanced scan shows spindle-shaped ring enhancement adjacent to the left side of the falx cerebri, with a reduction in size compared to the previous scan. (B) T2 sequence shows a high fusiform signal at the left side of the falx of the brain, which is smaller than before, and the primary peripheral cerebral edema is basically dissipated.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.