
Figures & data
Figure 1 The flow chart of the study. The criteria of possible IPA: (1) Patients’ age ≥18; (2) immune insufficiency (such as congenital immunodeficiency, long-term glucocorticoid treatment (glucocorticoid treatment time ≥3 weeks in the past 60 days),Citation13 long-term immunosuppressive therapy after solid organ transplantation, radiotherapy and chemotherapy for malignant tumors, etc) or others with emerging risk factors of IPA, such as end-stage COPD, liver cirrhosis, etc; (3) The time for appearance of suspected clinical symptoms or abnormal imaging manifestations of IPA was ≤1 month; (4) abnormal infiltrative manifestations in pulmonary CT images. On the basis of the possible IPA, proven IPA criteria should also meet: histopathological evidence or positive culture result from sterile environment (excluding BALF), probable IPA criteria should meet: mycologic evidence such as GM test, positive culture result (qualified specimen from sputum, BALF, bronchial brush), Aspergillus PCR, etc.
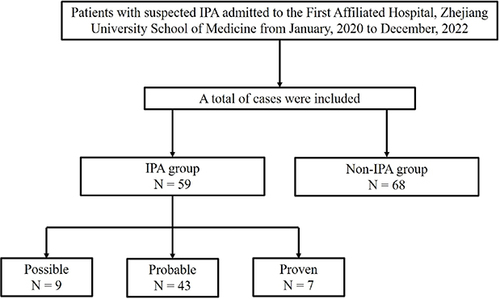
Table 1 Clinical Baseline Information of IPA and Non-IPA Patients
Table 2 Laboratory Testing Results of IPA and Non-IPA Patients
Figure 2 (A) The level of Aspergillus fumigatus-specific IgG antibody in IPA and non-IPA patients. (B) The level of A. fumigatus-specific IgG antibody in possible, probable and proven IPA patients. ***p < 0.001.
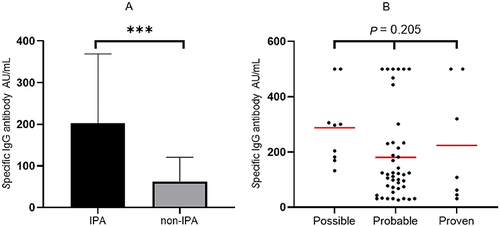
Table 3 Sensitivity and Specificity of Aspergillus fumigatus-Specific IgG Antibody Test at Different Cut-Offs in the Diagnosis of IPA
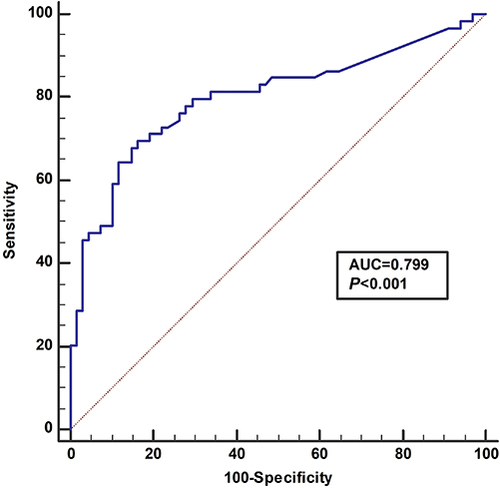
Figure 3 The ROC curve of Aspergillus fumigatus-specific IgG antibody test in the diagnosis of IPA.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.