Figures & data
Table 1 Patient’s laboratory data
Figure 1 Computed tomography (axial image, arterial phase) and endoscopic retrograde cholangiography findings. (A) Computed tomography imaging shows no mass lesion. (B) endoscopic retrograde cholangiography shows no stones in common bile duct and no extrahepatic biliary duct dilatation.
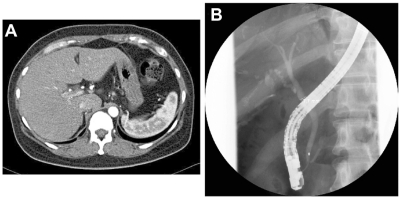
Figure 2 Light microscopic findings of liver biopsy. (A) Bile canalicular cholestasis findings showing edematous and pigmented hepatocytes around the central vein (arrowheads). “C” denotes the central vein. (B) Inflammatory infiltrate is made of polynuclear neutrophils and a varying number of eosinophils. Interlobular bile duct destruction is present in the portal tract. The arrow indicates destructive cholangitis. “P” denotes the portal vein. (C) HE and diastase-digested periodic acid-Schiff show intraepithelial neutrophilic infiltration in the interlobular bile duct. (D) Silver staining shows that basement membrane of the bile duct is preserved, but the nuclear arrangement is irregular. (E) Masson’s trichrome staining yields no evidence of portal fibrosis. (F) Cytokeratin 7 immunostaining shows positive cytoplasmic expression in the bile duct.
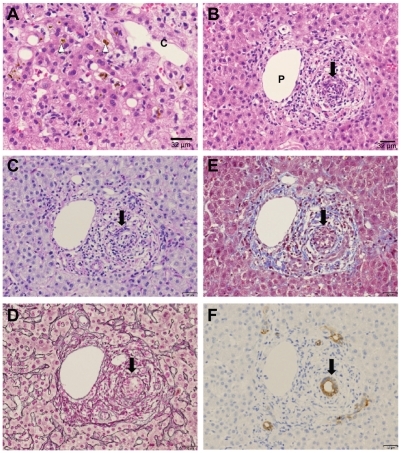
Figure 3 Electron microscopic findings. (A) Degenerative bile duct-related epithelial cells (arrowhead) are in an apoptotic process, as inferred from the appearance of condensed polymorphic and fragmented nuclei. The intercellular space adjacent to this degenerative epithelium is remarkably dilated (arrow), implying that bile substances are regurgitated from the lumen to the abluminal side. (B) A canal of Hering (CoH) with markedly dilated lumen (L) and loss of microvilli is lined by two hepatocytes (H1 and H2) and four cholangiocytes (C1–C4) containing deposits of electron-dense biliary substances (arrowhead). The intercellular space adjacent to epithelium is dilated (arrow). Between the two hepatocytes (H1 and H2) is a remarkably dilated bile canaliculus (BC) showing complete loss of microvilli and heavy deposition of biliary substances (arrow). (C) This electron micrograph shows a pseudo-bile ductule, the lumen of which is lined by six hepatocytes containing bile substances. The adjacent bile canaliculus (BC) is dilated with loss of microvilli and deposit of bile substances. The arrow indicates deposition of biliary substances.
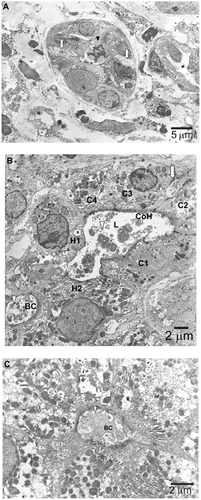
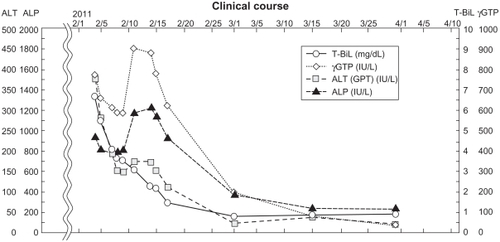
Figure 4 Clinical course.