Figures & data
Figure 1 Results of weekly phosphate (Pi) removal by hemodialysis (HD) and continuous ambulatory peritoneal dialysis (CAPD) procedures. The amount of Pi removed weekly by HD sessions three times a week was 2388–3006 mg/week in eleven patients. The removal by CAPD with residual kidney function was 2300 ± 113 mg/week in 13 patients, less than that by HD. These amounts of Pi removed by conventional dialysis therapy alone are insufficient, and this is why a Pi binder is used.
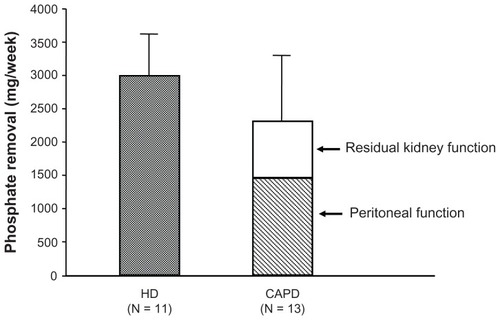
Figure 2 Lanthanum carbonate effectively controls serum phosphate (Pi) in a dose-dependent manner. The result was obtained from the prospective, randomized, double-blind, placebo-controlled, multicenter study on Japanese hemodialysis patients. Changes in serum Pi level from week –3 to week 6 are presented for each treatment group, together with the last observation carried forward as the endpoint. Lanthanum carbonate effectively controls serum Pi without affecting serum calcium level. The magnitude of serum Pi level reduction is greater at higher dosages, but it reached a plateau at a daily dose of 2250 mg.
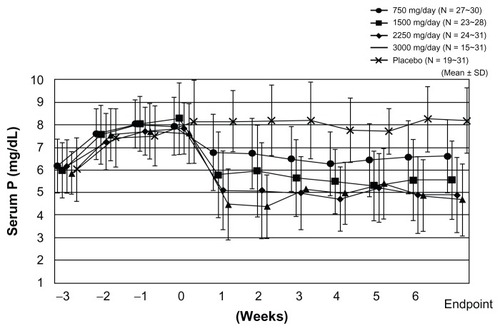
Figure 3 Correlation between the calcium (Ca)-phosphate (Pi) product and the serum Ca or serum Pi concentration. The serum Pi level was the significant factor in determining CaPi product. The CaPi product is mainly determined by the Pi concentration and is closely correlated with the serum Pi (Y = 10.476 – 5.155, r2 = 0.914), but not with the serum Ca (r2 = 0.229).
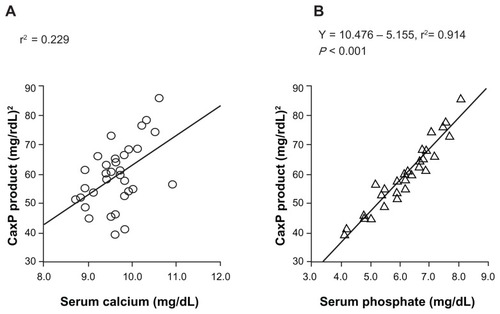
Figure 4 Prospective, randomized, double-blind, multicenter comparative study between lanthanum carbonate and calcium (Ca) carbonate as phosphate (Pi) binder in hemodialysis patients with hyperphosphatemia. In the lanthanum carbonate group, the mean serum Pi level decreased from 8.35 mg/dL at baseline to 5.78 mg/dL at week 5, and the serum Pi level was maintained up to the last visit. (A) A similar decrease in serum Pi level was also observed in the Ca carbonate group. During the double-blind period, the corrected serum Ca levels in the Ca carbonate group gradually increased, while those in the lanthanum carbonate group were relatively constant. (B) The daily doses of lanthanum carbonate became relatively constant during the last 4 weeks. At the last visit, the daily doses of lanthanum carbonate and Ca carbonate were 1725.7 and 3430.4 mg/day, respectively (C).
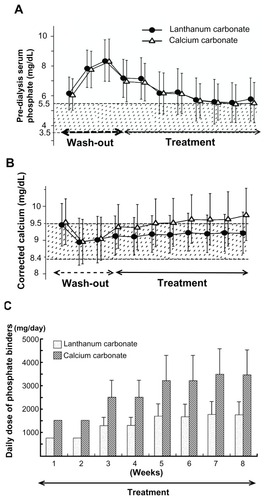
Figure 5 Clinical effects of 3-year extension study of lanthanum carbonate therapy in Japanese hemodialysis patients. (A) The mean serum phosphate (Pi) level was 8.03 ± 1.51 mg/dL at baseline, and it decreased to 5.33 ± 1.27 mg/dL and 5.33 ± 1.04 mg/dL after 1 year and 3 years of treatment, respectively. The mean reduction of Pi from baseline was within the range of –1.51 ± 1.48 mg/dL in week 1 (95% CI: −1.76, −1.27) to −3.08 ± 1.76 mg/dL in week 128 (95% CI: −3.69, −2.47). (B) The calcium (Ca)-Pi product has been well controlled below 55.0 (mg/dL)2 dependent on serum Pi level. (C) On the other hand, the intact parathyroid hormone (PTH) level was elevated overall and then stable throughout the treatment period, with a median value of 262.0 pg/mL at baseline and 283.8 pg/mL at 3 years.
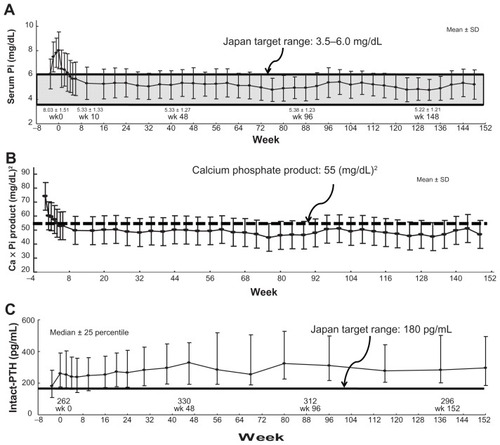
Figure 6 Effect of lanthanum carbonate treatment on bone in Japanese dialysis patients with hyperphosphatemia. In seven patients, pretreatment diagnosis was a fibrous osteitis–type disorder in two patients, a milder-type disorder in three patients, and an adynamic bone disease (ABD)–type disorder in two patients. After 1 year of treatment, the diagnosis changed to a milder-type disorder in all seven patients. After 3 years of treatment, bone biopsy was conducted on a total of four patients. The diagnosis of a milder-type disorder was maintained in all four patients. The results of histomorphometric analysis of cancellous bone showed that lanthanum carbonate treatment improved the osteoid condition toward normalization both in cases of excessive and cases of insufficient osteoid, and that the treatment also improved the resorption condition toward normalization in cases with both enhanced and reduced resorption.
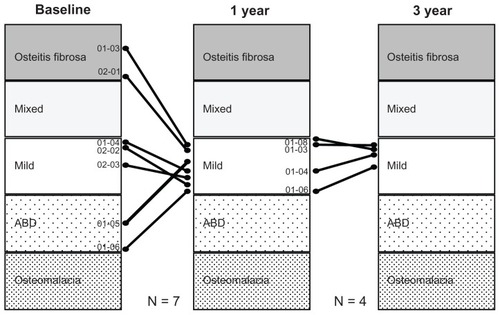
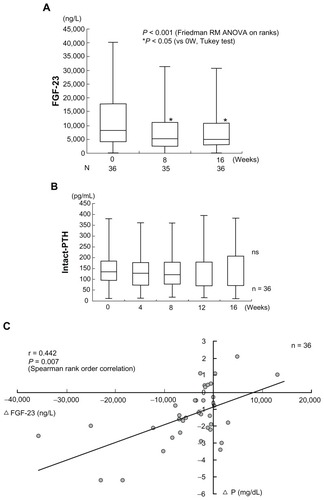
Figure 7 Combined therapy with lanthanum carbonate and calcium (Ca) carbonate for hyperphosphatemia decreases serum FGF23 levels independently of Ca and parathyroid hormone (PTH). The horizontal bar in each box indicates the median value. Upper and lower borders of the box are the 25th and 75th percentiles, respectively. Maximum and minimum values are shown by the vertical error bars. The significant 40% reduction of the circulating intact FGF23 level from baseline was observed after week 8 and week 16 of combined therapy of lanthanum carbonate and Ca carbonate therapy. On the other hand, the intact PTH level did not show any significant change within 16 weeks.