Figures & data
Figure 1 (A) Large staghorn calculus occupying the right renal pelvis with extension into the calyces in a case of confirmed XGP. (B) IVP in a different patient showing absent excretion in the affected upper pole and normal excretion in the unaffected lower pole (more horizontal arrow). A large irregular calculus is also evident immediately caudal to the right transverse process of L3 (more vertical arrow). The larger drain further caudally is in a psoas abscess and was inserted from the groin.
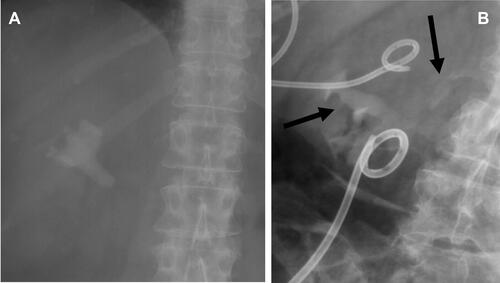
Figure 2 (A) Fluoroscopic image following contrast injection via a nephrostomy catheter demonstrating opacification of a psoas abscess cavity (white arrow) via a sinus from the pyeloureteric junction and opacification of multiple abscess-cutaneous sinuses in the groin (black arrows). (B) Digital subtraction pyelography during contrast injection of a nephro-ureteral stent in the same patient demonstrating opacification of a psoas abscess cavity via a sinus (black arrow) at the level of the pyeloureteric junction. Markedly scarred, ragged calyces and a severely contracted renal pelvis are evident in the affected upper pole moiety.
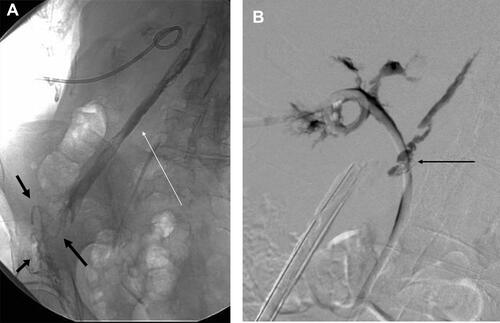
Figure 3 (A) Ultrasound of the kidney showing an “ultrasound bear-paw” with a central calculus and infiltrated fat and dilated, infiltrated calyces peripherally. The overlying cortex is chronically thinned. (B) Further ultrasound image in the same patient showing more marked calculous shadowing and a multilocular extrarenal collection (arrows).
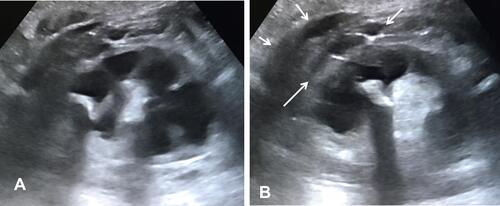
Figure 4 (A) Transaxial CT post-intravenous contrast showing multiple rounded low-attenuation foci converging on a dense calculus in a contracted renal pelvis in a “bear paw” configuration. Extrarenal extension is also evident, more conspicuous in (white arrow) (Elder & Malek Stage 3 disease). (B) Extrarenal extension involving the posterior pararenal space, transversalis and deep intercostal musculature, with a small abscess cavity at the interface between transversalis and intercostal musculature (white arrow), abutting, but not eroding the rib. The posterior perirenal fascia (Zuckerkandl’s) is completely engulfed. Thickening of the lateral conal and anterior perirenal fasciae and dense stranding of the properitoneal fat plane is evident (Elder & Malek Stage 3 disease).
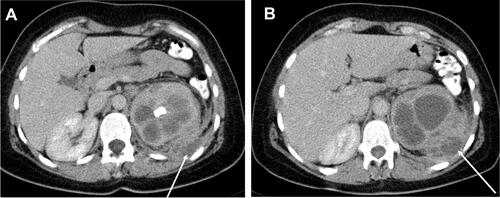
Figure 5 (A) Segmental XGP affecting the upper pole of the right kidney showing infiltrated calyces centred on a staghorn calculus in a bear-paw configuration (Elder & Malek Stage 1 disease). (B) Entirely normal lower pole moiety in the same patient.
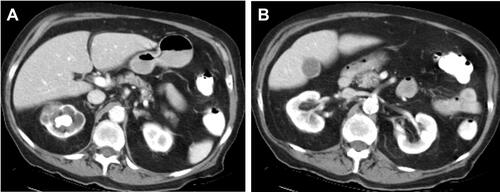
Figure 6 Multiple hypodense locules with the caudal fibres of the expanded right iliacus muscle (black arrows) representing an abscess arising from XGP in the right kidney (note the marked asymmetry with the normal left iliacus) (Elder & Malek Stage 3 disease). Bubbles of gas are shown in the right inguinal region at the site of multiple secondary cutaneous sinuses (white arrow). Contrast is also visible within the sinuses following contrast sinography.

Figure 7 MAG 3 of a 64-year-old lady with XGP in the upper pole of a duplex right kidney, showing loss of function in the affected pole, but with preserved function in the lower pole moiety, the latter accounting for 38% of total renal function. Subsequent management was directed at preserving the lower pole and managing the complications relating to the upper pole. These goals were achieved using antibiotics and percutaneous interventions only.

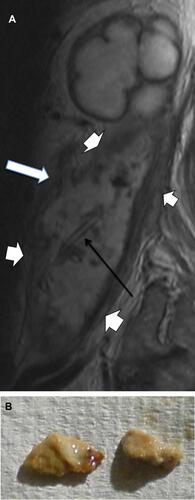
Figure 8 (A) MRI showing grossly distended calyces in the upper pole and a complex abscess cavity with a dramatically thickened, infiltrative wall (short white arrows) and innumerable foci of contained debris. The abscess arose secondary to erosion of irregular calculi through the renal pelvis, creating a sinus (long white arrow). A drainage catheter is evident within the abscess cavity (black arrow), placed via an accessed open sinus in the groin. (B) Two of the calculous fragments extracted from the abscess cavity via the groin.