
Figures & data
Table 1 Comparisons of BP Target Ranges and Recommendations for Drug Treatment in KDIGO CKD 2012, JSN CKD 2018, ESC/ESH 2018, and ACC/AHA 2017
Figure 1 Mechanisms of hypertension induced by renal parenchymal damage.
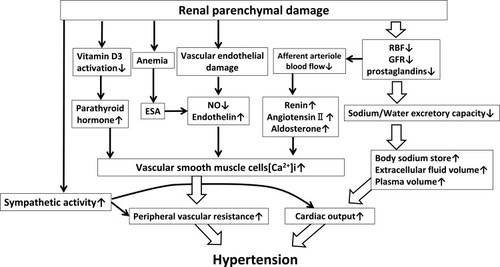
Table 2 BP Treatment Target Ranges of JSN CKD 2018
Figure 2 Hypothetical mean arterial blood pressure (BP) and intra-glomerular BP curves when using RAS inhibitors. In the absence of arteriosclerosis, if the mean systemic arterial pressure drops from (A) 160 mmHg to (B) 80 mmHg, the decrease in glomerular pressure is small (white arrow). However, if the atherosclerotic change is severe, there would be an insufficient increase in glomerular pressure due to dilation of efferent arterioles induced by RAS inhibitors, and the mean arterial pressure decreases rapidly (a’ to b’), causing glomerular pressure to drop sharply (black arrow).
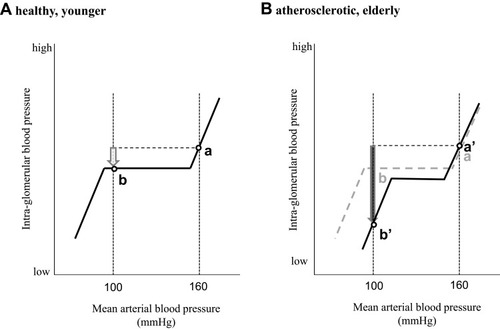
Figure 3 Meta-analysis results of the composite renal endpoints of EMPA-REG outcome, CANVAS, DECLARE-TIMI 58 and CREDENCE. The composite renal endpoints were significantly suppressed by SGLT2 inhibitors, regardless of baseline renal function. These meta-analyses were performed using RevMan 5 software (Cochrane, London, UK). The analyses were performed regardless of renal function (A) and limited to eGFR ≤60 mil/min/1.73 m2 (B). The results show that renal composite endpoints are significantly suppressed, regardless of baseline renal function or if eGFR is limited <60 mL/min/1.73 m2.
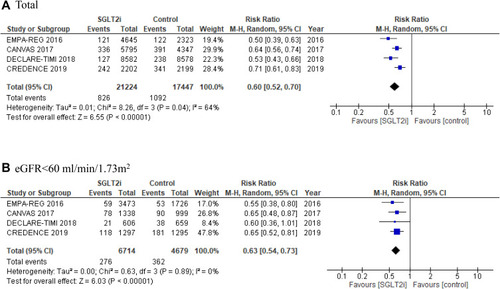
Table 3 Randomized Clinical Trials of Sodium-Glucose Cotransporter-2 Inhibitors