
Figures & data
Table 1 Clinical Characteristics of Patients and Encounters
Figure 1 Relationship of paired SCV CI to IVC CI values for encounters determined for all data (A), and different subgroups including transverse versus longitudinal SCV views (B), ventilated versus non-ventilated encounters (C), no central venous (CV) access versus CV access versus arterio-venous fistula (AVF) versus other* (peritoneal dialysis access (n=6) or femoral access (n=2)) (D), and AKD versus AKD on CKD versus ESKD (E). The IVC CI cut-offs of 20% and 50% are indicated by vertical-dotted lines.
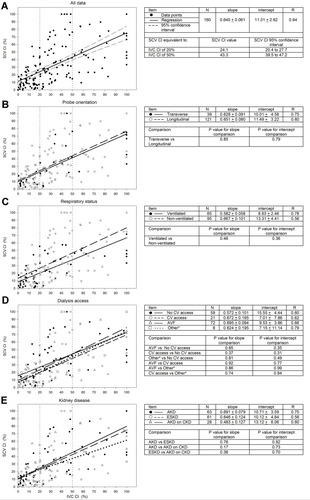
Figure 2 Sensitivity and specificity plots for various SCV CI cut-offs as predictors for whether IVC CI is <20% or >50% for spontaneous breathing and ventilated encounters. Solid circles are sensitivity and open circles are specificity. The solid lines are the sigmoidal fit to the data constrained to maximum and minimum sensitivities and specificities of 100% and 0%, respectively. The SCV CI cut-off at which the sensitivity and specificity are equal is indicated by the vertical lines. Sensitivity and specificity plots for various SCV CI cut-offs as predictors for whether IVC CI is <20% for spontaneous breathing encounters (A), <20% for mechanically ventilated encounters (B), >50% for spontaneous breathing encounters (C), >50% for mechanically ventilated encounters (D). Sensitivity and specificity plots for various SCV CI cut-offs from data derived from published reports, as predictors for whether IVC CI is <20% for spontaneous breathing encounters for medical patients (Munir et alCitation16) (E), <20% for spontaneous breathing and mechanically ventilated encounters for surgical ICU patients (Kent et alCitation13) (F), >50% for spontaneous breathing encounters for medical patients (Munir et alCitation16) (G), and >50% for a combination of spontaneous breathing and mechanically ventilated encounters for surgical ICU patients (Kent et alCitation13) (H). For the data from Munir et al,Citation16 collapsibility index ((max-min)/max) *100% was derived from (1-the ratio of min/max) for both SCV CI and IVC CI.
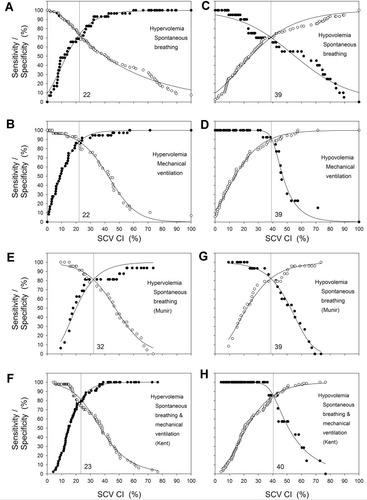
Table 2 Relationship of Subclavian Vein to Inferior Vena Cava Data for Our Study, and Comparison to Data Derived from Previous Studies