
Figures & data
Table 1 Tubular biomarkers
Figure 1 Characteristic histological features of diabetic nephropathy.
Notes: In advanced diabetic nephropathy, there is extensive mesangial expansion due to increased extracellular matrix production, with the formation of spherical, eosinophilic nodules with a central hypocellular or acellular area, known as Kimmelstiel–Wilson nodules (A) (hematoxylin–eosin, ×400). These nodules are also typically strongly periodic acid–Schiff-positive and may be seen compressing and narrowing the peripheral capillary loops (B) (periodic acid–Schiff, ×400). The increased matrix stains dark with silver and the Kimmelstiel–Wilson nodules may demonstrate a lamellated appearance. Capillary microaneurysms can be seen at the periphery on the right (in the 1–5 o’clock position), in association with mesangiolysis (C) (Masson’s trichrome–methenamine silver, ×400). There is diffuse thickening of the glomerular basement membrane, which is apparent on electron microscopy even if it is difficult to discern by light microscopy in early disease, and often accompanied by some degree of podocyte foot process effacement (D) (electron microscopy).
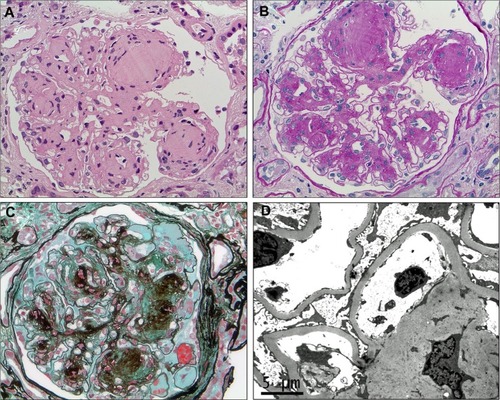
Figure 2 Overview of the pathological pathways in diabetic nephropathy.
Notes: In the diabetic milieu, metabolic derangements and hemodynamic alterations, particularly activation of the renin–angiotensin system, trigger a number of cell signaling cascades, including the MAPKs (p38 and JNK) and PKC-β, which mediate a cellular response through activation of key transcription factors such as NF-κB. In response to such signals, renal cells such as tubular epithelial cells, podocytes, and mesangial cells can produce chemokines, growth factors, and profibrotic cytokines. CSF-1 and MCP-1 function as chemotactic molecules and promote the recruitment of monocytes from the circulation. Upregulation of ICAM-1 on endothelial cells – a key leukocyte adhesion molecule – facilitates infiltration of circulating mononuclear cells into the kidney. CSF-1 also promotes monocyte/macrophage differentiation, proliferation, and activation. MIF functions to retain macrophages at sites of inflammation and has counter-regulatory functions against the anti-inflammatory actions of glucocorticoids. Activated macrophages can produce proinflammatory and profibrotic cytokines, reactive oxygen species, and antiangiogenic factors and contribute to a cycle of inflammation, oxidative stress, cellular injury, progressive fibrosis, and loss of glomerular filtration rate. Podocyte loss, endothelial dysfunction, alterations in the GBM, and tubular injury contribute to increasing proteinuria during the development and progression of diabetic nephropathy.
Abbreviations: AGE, advanced glycation end-products; GBM, glomerular basement membrane; GFR, glomerular filtration rate; Mac, macrophages; Mon, monocyte; NOS, nitric oxide synthase; ROS, reactive oxygen species.
Abbreviations: AGE, advanced glycation end-products; GBM, glomerular basement membrane; GFR, glomerular filtration rate; Mac, macrophages; Mon, monocyte; NOS, nitric oxide synthase; ROS, reactive oxygen species.
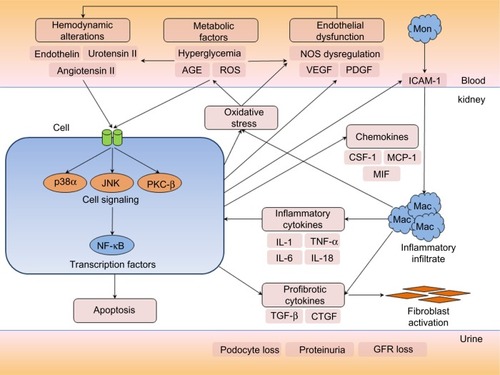
Figure 3 Macrophages in diabetic nephropathy.
Notes: Immunostaining for a macrophage marker (CD68) in kidney sections shows sparse interstitial macrophages in age-matched, nondiabetic control mice (A) compared to diabetic mice after 20 weeks of diabetes induced by streptozotocin (B) (CD68 brown, counterstained with hematoxylin, ×250).
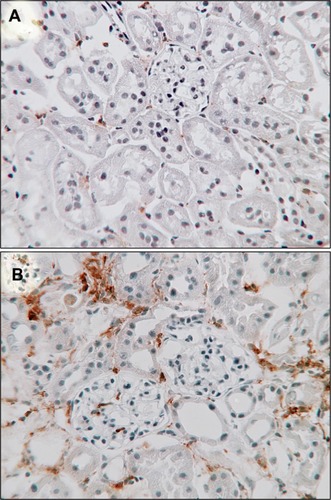
Table 2 Summary of pharmacological treatment of diabetic nephropathy
Table 3 Diet and alternative medicine
Table 4 Summary of novel agents
Table 5 Stem cell therapy in experimental diabetic nephropathy