Figures & data
Figure 1 (A–E) Clinical manifestations of hereditary leiomyomatosis and renal cell carcinoma (HLRCC): leiomyomas.
Notes: (A) Multiple cutaneous leiomyomas on the torso of an HLRCC patient. (B) Histomicrograph of cutaneous leiomyoma, showing interlaced bundles of smooth-muscle fibers with a centrally located long, blunt-edged nucleus. (hematoxylin and eosin, [H&E] 10×). (C) Computed tomography image showing multiple large uterine leiomyomas (white arrows) that occur in most women with HLRCC, and that can be symptomatic. (D and E) High-power image of a uterine leiomyoma showing large prominent nuclei with an orangiophilic nucleolus (white arrows) surrounded by perinuclear halo; H&E, 300× and 400×. Images from Grubb et alCitation32 (A and C), Rothman et alCitation54 (B), and Sanz-Ortega et alCitation30 (D and E).
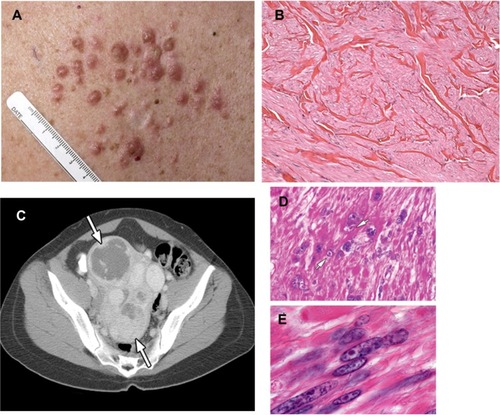
Figure 2 (A–E) Clinical manifestations of hereditary leiomyomatosis and renal cell carcinoma (HLRCC): renal tumors.
Notes: Computed tomography images showing (A) para-aortic nodal disease (white arrow) and (B) left renal tumor (white arrow) in HLRCC patients. RCC in HLRCC patients may present with (C) papillary morphology suggestive of type 2 papillary RCC (10×), but (D) tubular and cystic patterns may also be seen (10×). (E) Under high power, the characteristic orangiophilic or eosinophilic nucleoli with perinuclear halo are seen (40×). Images from Grubb et al.Citation32
Abbreviation: RCC, renal cell carcinoma.
Abbreviation: RCC, renal cell carcinoma.
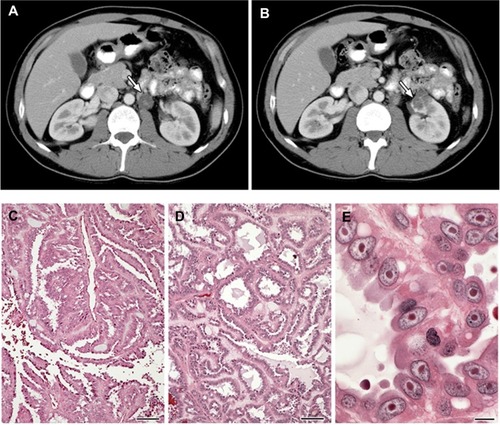
Table 1 Diagnostic criteria for hereditary leiomyomatosis and renal cell carcinoma (HLRCC)
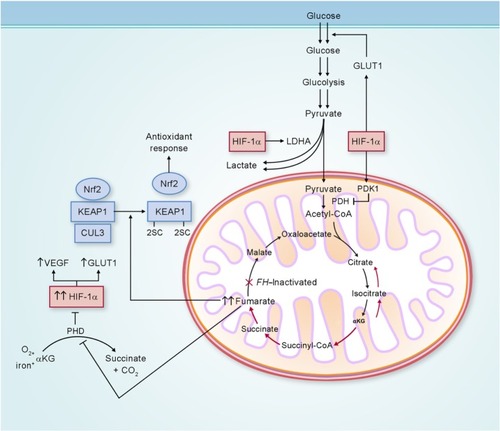
Figure 3 Potential biochemical pathways deregulated as a consequence of FH inactivation.
Notes: FH-deficient kidney cancer has impaired oxidative phosphorylation, and undergoes a metabolic shift to aerobic glycolysis to generate adenosine triphosphate for cellular energy demands. Fumarate, which accumulates in FH-deficient cells, can competitively inhibit prolyl hydroxylase (PHD), resulting in HIF-1α stabilization and increased expression of the HIF-1α target genes VEGF and GLUT1. Elevated fumarate also succinates KEAP1, altering its conformation and inhibiting its ability to degrade nuclear factor erythroid 2-related factor 2 (Nrf2). Nrf2 transcriptional activity is upregulated, leading to activation of the antioxidant-response pathway and protection against oxidative stress. Adapted from Linehan and Rouault.Citation21
Abbreviations: LDHA, lactate dehydrogenase A; CoA, coenzyme A; αKG, α-ketoglutarate; FH, fumarate hydratase; GLUT1, glucose transporter 1; KEAP1, kelch-like ECH-associated protein 1; CUL3, cullin 3; HIF-1α, hypoxia-inducible factor 1 alpha; VEGF, vascular endothelial growth factor; PDH, pyruvate dehydrogenase; PDK1, pyruvate dehydrogenase kinase 1.
Abbreviations: LDHA, lactate dehydrogenase A; CoA, coenzyme A; αKG, α-ketoglutarate; FH, fumarate hydratase; GLUT1, glucose transporter 1; KEAP1, kelch-like ECH-associated protein 1; CUL3, cullin 3; HIF-1α, hypoxia-inducible factor 1 alpha; VEGF, vascular endothelial growth factor; PDH, pyruvate dehydrogenase; PDK1, pyruvate dehydrogenase kinase 1.