
Figures & data
Figure 1 Age-specific IR per 100,000 py for the most common types of hyperthyroidism in Denmark (Graves’ disease, multinodular toxic goiter, and solitary toxic adenoma).
Abbreviations: IR, incidence rate; py, person-years.
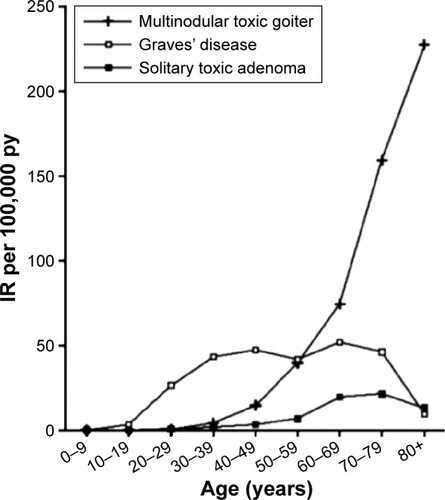
Figure 2 IR of maternal hyperthyroidism in 3-month intervals before, during, and after the first pregnancy leading to birth of a live-born child from 1999 to 2008 in a Danish population-based study of 403,958 women.
Abbreviation: IR, incidence rate.
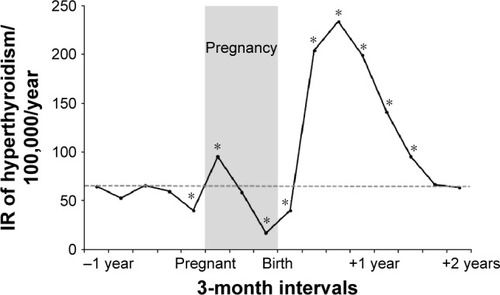
Figure 3 Reference limits for the diagnosis of hyperthyroidism in early pregnancy established with the Dimension Vista (Siemens) automatic immunoassay.
Abbreviations: TSH, thyroid-stimulating hormone; CI, confidence interval; fT4, free T4.
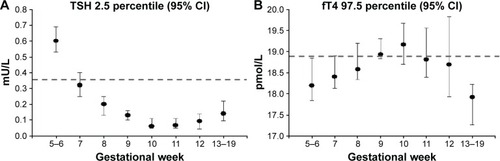
Figure 4 Adjusted OR with 95% CI for subtypes of birth defects in 1,097 children exposed to MMI/CMZ and 564 children exposed to PTU in early pregnancy versus the reference group of 811,730 children not exposed to ATD.
Abbreviations: OR, odds ratio; CI, confidence interval; MMI, methimazole; CMZ, carbimazole; PTU, propylthiouracil; ATD, antithyroid drug.
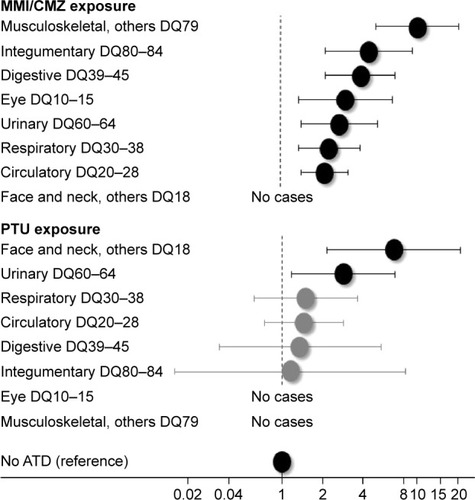
Table 1 Proposals on the treatment of hyperthyroidism in women who are or plan to become pregnant