Figures & data
Figure 1 A pre-contrast axial CT image showed a homogeneously cystic lesion of the pancreatic body and tail. A single focus of punctate calcification (arrowhead) is present in the region of the pancreatic tail that does not contact the cyst wall. No hyperattenuating content was seen within the cyst.

Figure 2 Coronal (A) and sagittal (B) views of the portal venous phase revealed a large (18.4 cm x 17.7 cm x 12 cm) thin-walled, lobulated, and trans-spatial lesion (white arrowheads in B). It did not show any internal enhancement, mural nodularity, septations, or signs of local organ invasion. As it extended posterosuperiorly to the left subdiaphragmatic space, the lesion assumed a C-configuration. It pushed the spleen inferiorly (black arrowhead in B) and squeezed the stomach (black arrow in A and B).
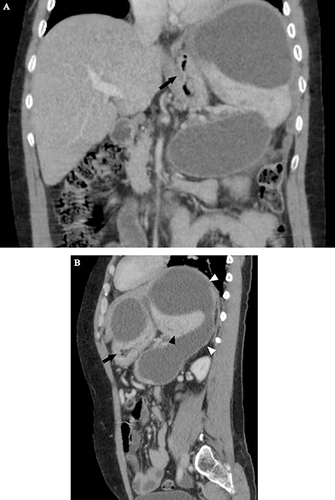
Figure 3 Arterial (A, C) and portal (B) phase axial images showed a well-opacified tortuous splenic artery at the splenic hilum (black arrowhead in A). The proximal portion was also well opacified, with no evidence of a filling defect. The portal phase showed multiple non-enhanced tubular structures (white arrowhead in B) in the expected location of the splenic vein, signifying chronic splenic vein thrombosis. More inferiorly, inflammatory stranding was seen in the left perinephric space, with prominent left anterior renal and lateroconal fasciae (white arrow in C). Along the left peritoneal surface, a smaller but similar cystic lesion was visible (black arrowhead in C). Multiple non-enhancing splenic cysts were evident.

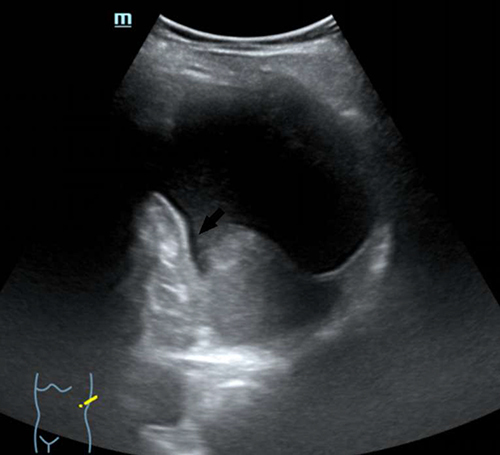
Figure 4 An oblique left quadrant B-mode abdominal sonography three months after the initial CT scan showed an inferiorly displaced spleen with a 7.3 cm x 7.2 cm left subdiaphragmatic cystic lesion that showed an increased posterior through transmission and a beak-like linear extension to the splenic hilum region (black arrow). The pancreas, as well as the lesser sac space, were free of cystic areas. The splenic cystic lesions were also resolved.