Figures & data
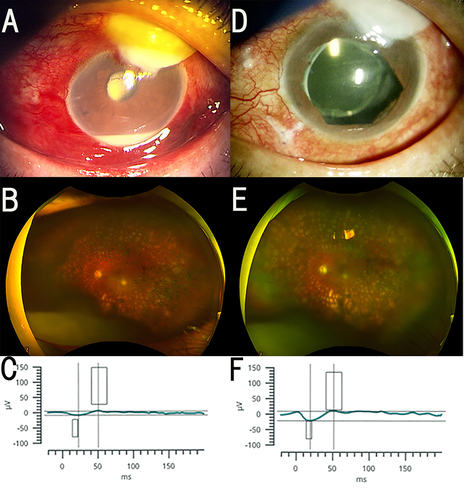
Figure 1 Case 1. This patient developed exogenous endophthalmitis after undergoing trabeculotomy. Slit-lamp images, fundus photographs, optical coherence tomographic (OCT) images, and electroretinograms (ERGs) before and during the bleb-associated endophthalmitis are shown. (A) Slit-lamp image on the initial visit showing an avascular bleb, conjunctival hyperemia, and a mild upper corneal opacity. (B) Fundus photograph 1 day before the surgery showing that the fundus was not visible due to vitreous opacity. (C) Mixed rod-cone electroretinogram (ERG) on the initial visit. The a- and b- wave amplitudes are moderately attenuated. (D) Slit-lamp image 2 weeks after surgery showing reduced height of the avascular bleb and slightly decreased injection. (E) Fundus photograph 4 days after surgery showing an intact retinal circulation and pale optic disc. (F) Mixed rod-cone ERG 3 days after the surgery. The a- and b-wave amplitude is larger than the preoperative values, and the b/a ratio is not changed at approximately 2.0 postoperatively. The implicit time of both waves was not altered. Note that the vertical axis representing the amplitude has a different scale.
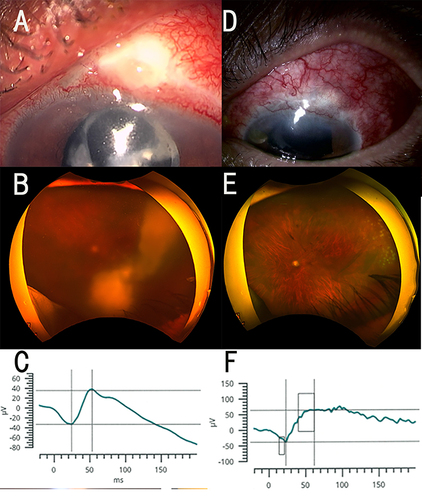
Figure 2 Case 2. Slit-lamp images, fundus photographs, optical coherence tomographic (OCT) images, and electroretinograms (ERGs) before and during the course of the bleb-associated endophthalmitis. (A) Slit-lamp image on the initial visit showing an avascular bleb, conjunctival hyperemia, and mild upper corneal opacity. (B) Fundus photograph 2 day before surgery showing relatively intact fundus before the exacerbation of an endophthalmitis. The fundus photograph was not taken due to opacified media on the following day. (C) Mixed rod-cone ERG on the initial visit. The a- and b- wave amplitudes are markedly reduced. (D) Slit-lamp image 2 weeks after the vitrectomy with irrigation containing 0.025% povidone iodine. Image shows white avascular bleb and decreased injection. (E) Fundus photograph 4 days after surgery showing an intact retinal circulation and pale optic disc. (F) Mixed rod-cone ERG 6 days after surgery. Compared to the preoperative response, the a- and b-wave amplitudes are larger, and the b/a ratio has not changed at approximately 1.5. The implicit times of both waves are not significantly changed.