
Figures & data
Figure 1 Angle and fundus findings before and after minimally invasive direct internal cyclopexy in case 1. (A) Preoperative gonioscopy in the nasal angle. The red arrow indicates a post-goniotomy cyclodialysis cleft of about 90°. (B) Preoperative anterior segment optical coherence tomography (AS-OCT) in the horizontal direction confirming the presence of a cleft (red arrow) along with a 360-degree ciliochoroidal detachment (white arrow). Anterior chamber-superior choroidal space traffic is clear. (C) Preoperative fundus camera image showing mild dilation and vascular tortuosity. (D) Preoperative OCT showing chorioretinal folds, which indicates hypotony maculopathy. (E) Postoperative gonioscopy finding in the nasal angle. The cyclodialysis cleft is repaired. Scattered peripheral anterior synechiae formations are visible after the cyclopexy. (F) Postoperative AS-OCT in the horizontal direction confirming repair of the cleft and disappearance of the ciliochoroidal detachment. (G) Postoperative fundus camera image showing mild dilation and vascular tortuosity are improved. (H) Postoperative OCT finding showing improved chorioretinal folds and the return of the retinal shape to normal, which indicates the resolution of hypotony maculopathy.
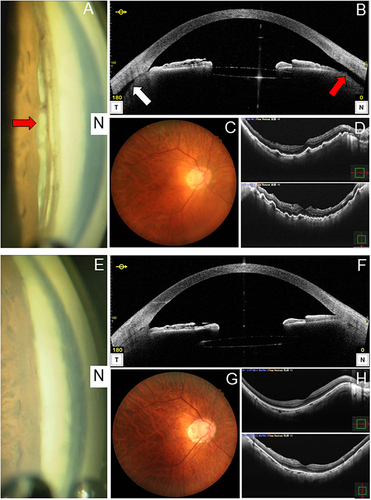
Figure 2 Angle and fundus findings before and after minimally invasive direct internal cyclopexy in case 2. (A) Preoperative 360-degree gonioscopic camera image. Red arrow indicates a post-goniotomy cyclodialysis cleft of about 45°. (B) Preoperative anterior segment optical coherence tomography (AS-OCT) in the horizontal direction confirming the disinsertion of the ciliary body from the scleral spur (red arrow) along with a shallow 360-degree ciliochoroidal detachment (white arrow). Anterior chamber-superior choroidal space traffic is not clear. (C) Preoperative fundus camera photo showing mild dilation and tortuosity of retinal veins. (D) Preoperative OCT showing chorioretinal folds, which indicates hypotony maculopathy. (E) Postoperative 360-degree gonioscopic camera image showing the cyclodialysis cleft is repaired. Scattered peripheral anterior synechiae formations after the cyclopexy are observed in the nasal angle. (F) Postoperative AS-OCT in the horizontal direction confirming the repair of the cleft and disappearance of the ciliochoroidal detachment. (G) Postoperative fundus camera image showing improvements in mild dilation and tortuosity of retinal veins. (H) Postoperative OCT showing improved chorioretinal folds and the return of the retinal shape to normal, which indicates the resolution of hypotony maculopathy.
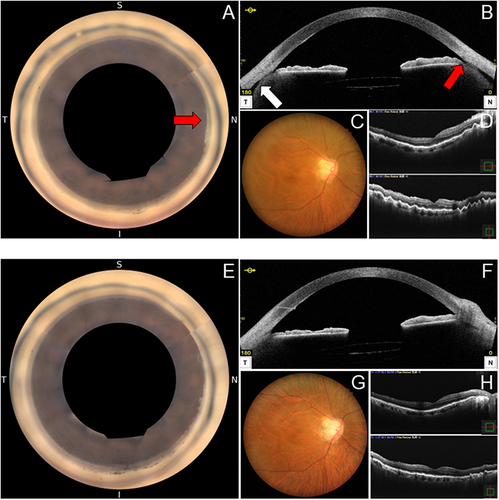
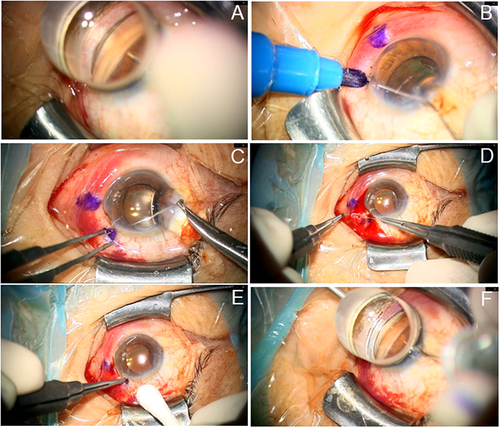
Figure 3 Continuous still images from the intraoperative video of minimally invasive direct internal cyclopexy being performed in case 2. (A and B) Confirmation and marking of the extent of cyclodialysis. (C) Intraocular insertion of PC-9 double needles into the ciliary sulcus at the site of cyclodialysis. (D) Mattress suture at the cyclodialysis site (internal direct cyclopexy). (E) Subconjunctival implantation of the knot. (F) Confirmation of the repair of cyclodialysis.
Data Sharing Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.