
Figures & data
Figure 1 CLL transformation into DLBCL.
Notes: (A) Large cells of DLBCL (lower left) next to infiltration by small CLL cells (upper right) HE, ×200 magnification. (B) DLBCL with centroblastic morphology (upper right); few small CLL cells (lower left); HE staining, ×400 magnification. (C) DLBCL cells reveal stronger membrane CD20 expression than that of CLL cells. (D) MIB1 staining in 80% of the DLBCL cells and in 3% of the CLL cells. (E) CD23 membrane expression in CLL cells; DLBCL cells are negative. (F) BCL6 nuclear expression in DLBCL cells; CLL is negative; EnVision staining, ×400 magnification.
Abbreviations: CLL, chronic lymphocytic leukemia; DLBCL, diffuse large B-cell lymphoma; HE, hematoxylin and eosin.
Abbreviations: CLL, chronic lymphocytic leukemia; DLBCL, diffuse large B-cell lymphoma; HE, hematoxylin and eosin.
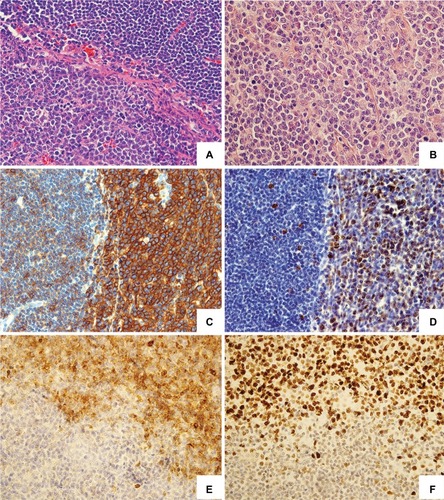
Figure 2 Morphological and phenotypic spectrum of CLL transformation into HL may strongly differ upon histopathological examination.
Notes: Type I – CLL with Hodgkin transformation (A–C). (A) Reed–Sternberg cells are sparsely dispersed in the background of small CLL cells; HE staining. (B) CD15 membrane and “dot-like” expression in HRS cell. (C) CD23 expression in CLL cells; the Reed–Sternberg cell is negative. EnVision staining, ×400 magnification. Type II – CLL transformation in HL (D–F). (D) The numerous HRS cells among histiocytes, eosinophils, and small lymphocytes in the background; a few CLL cells in the lower right; HE staining, ×200 magnification. The HRS cells reveal membrane CD30 expression (E) and “dot-like” expression of CD15 (F); EnVision staining, ×400 magnification.
Abbreviations: CLL, chronic lymphocytic leukemia; HE, hematoxylin and eosin; HL, Hodgkin’s lymphoma; HRS cell, Hodgkin and Reed–Sternberg cell.
Abbreviations: CLL, chronic lymphocytic leukemia; HE, hematoxylin and eosin; HL, Hodgkin’s lymphoma; HRS cell, Hodgkin and Reed–Sternberg cell.
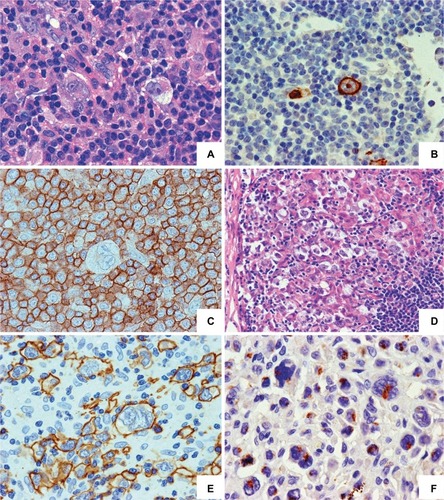
Figure 3 Management algorithm for patients with a clinical suspicion of RS.
Notes: In CLL patients characterized by chromosome 12 trisomy or NOTCH1 mutations, or classified as subset #8, and especially in those with the presence of constitutional symptoms or asymmetrical lymph node enlargement, caution is advised due to the increased risk of RS transformation. In case RS is suspected, a PET/CT should be performed and regions with SUV >5 were qualified for excisional biopsy. If the biopsy reveals no transformation, CLL treatment may be initiated. However, in cases with a strong suspicion of RS, a secondary biopsy should be considered. Once the histopathological diagnosis of RS-DLBCL is confirmed, a patient should be qualified for clonality assessment. In case of no clonal relationship between CLL and DLBCL, the patient should be treated as having de novo DLBCL. In contrast, for clonally related cases, the enrollment into clinical trial with novel compounds is advised due to poor prognosis with a standard immunochemotherapy. Fit and transplant-eligible patients with clonally related disease should be qualified for allogeneic stem cell transplantation or, if not possible, for autologous stem cell transplantation. In case of relapsed disease, platinum-based salvage regimens or participation in clinical trials is recommended. Transformation to Hodgkin’s lymphoma should be treated with ABVD regimen. Shading relates to administered therapies or treatment as final points of the algorithm. Other non-shaded fields represent the diagnostic activities and results.
Abbreviations: ABVD, adriamycin, bleomycin, vinblastine, and dacarbazine; CLL, chronic lymphocytic leukemia; DLBCL, diffuse large B-cell lymphoma; HSCT, hematopoietic stem cell transplantation; LDH, lactate dehydrogenase; PET/CT, positron emission tomography/computed tomography; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; RS, Richter syndrome; SUV, standardized uptake value.
Abbreviations: ABVD, adriamycin, bleomycin, vinblastine, and dacarbazine; CLL, chronic lymphocytic leukemia; DLBCL, diffuse large B-cell lymphoma; HSCT, hematopoietic stem cell transplantation; LDH, lactate dehydrogenase; PET/CT, positron emission tomography/computed tomography; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; RS, Richter syndrome; SUV, standardized uptake value.
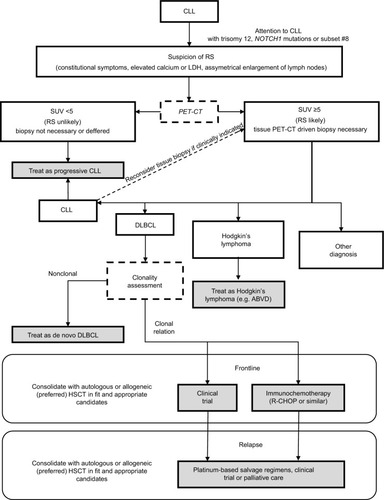
Table 1 Summary of the published retrospective studies assessing the efficacy and safety of induction regimens for patients with DLBCL-RS
Table 2 Summary of the published prospective studies assessing the efficacy and safety of induction regimens for patients with DLBCL-RS