Figures & data
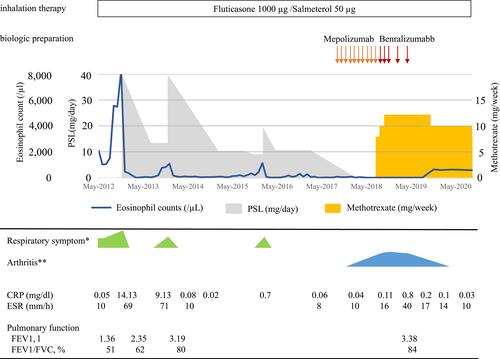
Figure 1 (A, B) Chest X-ray and chest CT scan in October 2012. Patchy infiltrations predominantly around the pleura with air bronchograms in the left upper lobe are seen. (C, D) Chest X-ray and chest CT scan in February 2013. Dramatic improvement is seen. (E, F) Chest X-ray and chest CT scan in April 2013. Relapse of CEP showing infiltration in right upper lobe is shown. (G) Chest X-ray in August 2015. Infiltrative shadow in left lower lung field is seen.
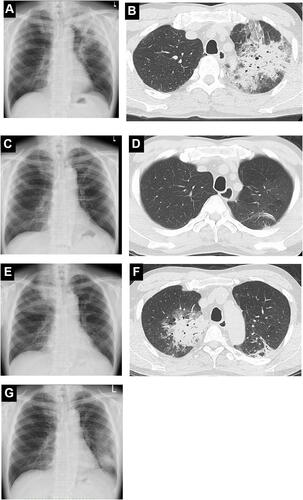
Figure 2 Clinical course of the patient. Oral prednisolone to control CEP was tapered off during mepolizumab therapy. Methotrexate was initiated for rheumatoid arthritis and mepolizumab was replaced by benralizumab. No exacerbations were noted after the discontinuation of benralizumab. The degree of respiratory symptom (*green) and arthritis (**blue) are indicated.