
Figures & data
Table 1 Underlying Conditions Associated with Acquired Hemophilia A
Figure 1 Mechanism of immune response to FVIII. FVIII is processed by the antigen-presenting cell (APC). Its function is to recognize and internalize it, giving rise to an endosome inside, which after merging with a lysosome leads to digestion of FVIII into peptide fragments that can bind to class II molecules of the major histocompatibility system. In case it is not assembled, the class II molecule will be degraded; otherwise, the complex will be transported to the surface of the APC, which presents it to the T cell receptor (TCR). The activation of T lymphocytes requires this union and the signals resulting from the interaction between various molecules such as CD28/B7 (pro-activation) or CTLA4/B7 (anti-activation). After this, there is an expansion of clone responsible for presenting FVIII to B lymphocytes. B lymphocytes (BL) are responsible for the production of specific antibodies (immunoglobulins [Ig]).
![Figure 1 Mechanism of immune response to FVIII. FVIII is processed by the antigen-presenting cell (APC). Its function is to recognize and internalize it, giving rise to an endosome inside, which after merging with a lysosome leads to digestion of FVIII into peptide fragments that can bind to class II molecules of the major histocompatibility system. In case it is not assembled, the class II molecule will be degraded; otherwise, the complex will be transported to the surface of the APC, which presents it to the T cell receptor (TCR). The activation of T lymphocytes requires this union and the signals resulting from the interaction between various molecules such as CD28/B7 (pro-activation) or CTLA4/B7 (anti-activation). After this, there is an expansion of clone responsible for presenting FVIII to B lymphocytes. B lymphocytes (BL) are responsible for the production of specific antibodies (immunoglobulins [Ig]).](/cms/asset/67adc884-78c0-4e71-9312-32e16b323ef6/djbm_a_12151116_f0001_c.jpg)
Figure 2 Kinetics of inhibition of FVIII activity by autoantibodies. The inhibition profile of FVIII activity which most often exhibit the autoantibodies characteristic in acquired haemophilia responds to a second order kinetics (triangles), in which a first phase of inhibition resulting from a linear pattern is followed by an equilibrium phase in which the inhibition rate slows markedly, a fact that allows the detection of residual FVIII activity in vitro. However, autoantibodies directed against FVIII rarely interact with this following a first-order kinetics (circles), in which the inhibition profile corresponds to a linear pattern and leads to the complete disappearance of FVIII activity, this being a more typical behavior of anti-FVIII alloantibodies that can occur in congenital haemophilia.
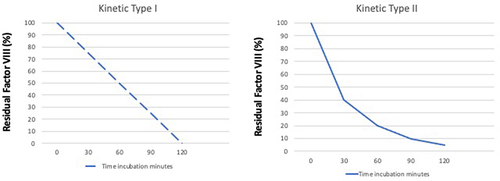
Figure 3 Examples of AHA bleeding profile. (A) Lingual and soft palate haematoma in patient with AHA. (B) Haemorrhagic infiltration of subcutaneous tissue due to abductor muscle bleeding in a patient with AHA.
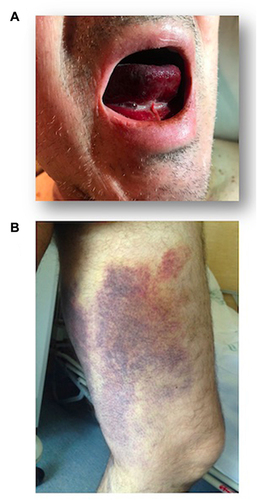
Figure 4 Diagnostic algorithm for a prolonged APTT. Kasper test and Bethesda assay requires incubation 2 hours at 37°C of the mixing samples. (1) No evidence of correction is defined as a test time 8 seconds longer than the control time.
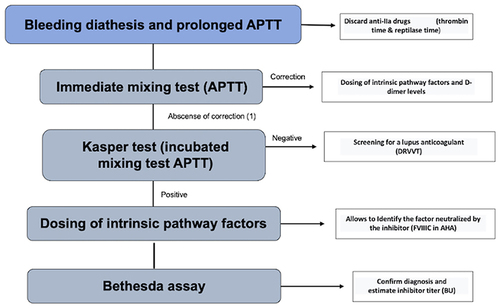
Table 2 Goals of AHA Treatment and Studies Recommended to Rule Out Underlying Conditions in Patients Suffering from AHA
Table 3 Suggested Surgical Prophylaxis in Adults with Acquired haemophiliaCitation94
Table 4 Outcomes of Immunosuppressive Treatment of Longest AHA Registries.Citation4–8,Citation113
Table 5 Cause of Mortality in Longest AHA Registries.Citation4–8,Citation113