
Figures & data
Table 1 The Baseline Characteristics of the Two Groups
Figure 1 RFA of a 68-year-old female with HCC abutting the gallbladder under intra-operative contrast-enhanced ultrasound (CEUS) monitoring. (A–C). Conventional ultrasound, CEUS and contrast-enhanced CT image showed HCC nodule in segment V abutting to the gallbladder with a maximum diameter of 22 mm (white arrow). Before ablation, the thickness of the gallbladder wall was 4 mm. (D) The electrode was inserted parallel to the gallbladder wall with a minimum distance of 6 mm (white triangle). (E) CEUS showed that the perfusion of the gallbladder wall was intact (red arrow) and the index tumor had been completely ablated (white arrow). (F) The thickness of the gallbladder wall increased to 10 mm one day after ablation (white triangle). (G) One month later, the contrast-enhanced MR confirmed the result of complete ablation (white arrow). (H) The thickness of the gallbladder wall was restored to 4 mm after 4 months on conventional ultrasound image (white triangle).
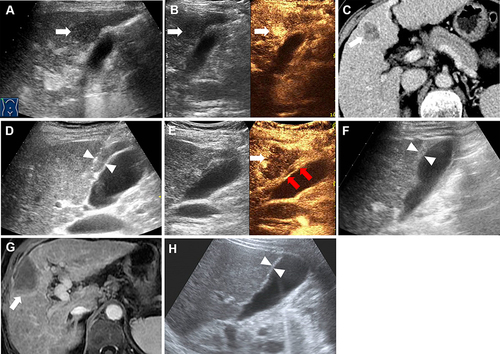
Figure 2 A 52-year-old male with HCC abutting the gallbladder underwent RFA with auxiliary artificial ascites. (A and C) Conventional ultrasound and contrast-enhanced MR image indicated a HCC lesion located in segment V abutting the gallbladder with a maximum diameter of 15 mm (white arrow). (A and B) Gallbladder stones were found on ultrasound images and the thickness of gallbladder wall was 4 mm. (D) Artificial ascites (white triangle) were employed to isolate the lesion and gallbladder before radiofrequency ablation. (E) The electrode (white arrow) was inserted parallel to the gallbladder wall. (F) After 4 ablation cycles, contrast-enhanced ultrasound showed that the index tumor had been completely ablated (white arrow). (G) One day after ablation, the thickness of the gallbladder wall increased to 7 mm (white triangle). (H) Contrast-enhanced MR one month after the ablation procedure confirmed the complete ablation of the index tumor (white arrow). (I) The thickness of gallbladder wall was restored to 4 mm after 5 months on conventional ultrasound image (white triangle).
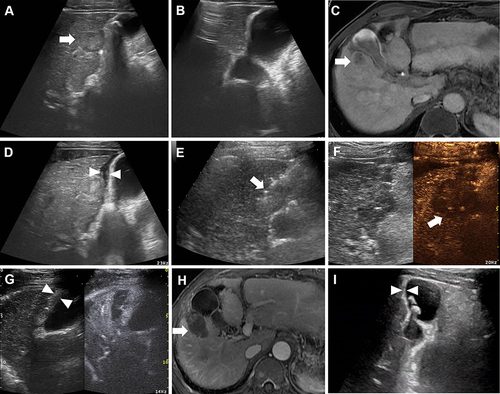
Figure 3 A 65-year-old male with cholelithiasis who was planned to undergo LC after RFA. (A–C) Conventional ultrasound and contrast-enhanced ultrasound (CEUS), and contrast-enhanced MR image showed a HCC (15×10 mm) in segment V abutting to the gallbladder (white arrow). Before ablation, the thickness of the gallbladder wall was 4 mm. (D) Sediment-like gallstones (white cross) were found on ultrasound images. (E) The electrode was inserted parallel to the gallbladder wall with a distance less than 5 mm (white cross). (F) CEUS showed that the index tumor had been completely ablated (white arrow) while the perfusion defect of the gallbladder wall was found by accident (red arrow). Patient underwent LC soon after RFA procedure, thermal damage of the gallbladder wall was found in postoperative specimens. (G) Postoperative pathology confirmed the thermal damage of the serosa and mucosa of the GB wall. (H) CEMR one month after the RFA procedure confirmed the technical efficacy (white arrow).
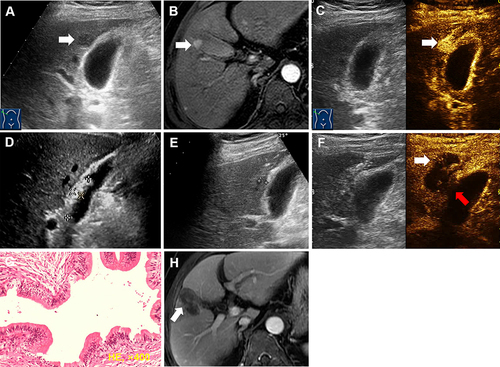
Table 2 Therapeutic Effect and Re-Treatment
Table 3 Cumulative LTP, IDR, OS and TFS Rates of Group A and Group B
Figure 4 Comparison of the cumulative local tumor progression (A), intrahepatic distant recurrence (B), overall survival (C) and tumor free survival (D) curves between group A and group B.
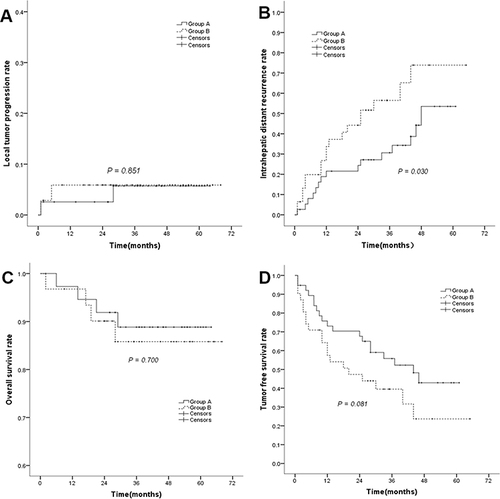
Table 4 Thickness of Gallbladder Wall