Figures & data
Figure 1 Diagram of study flow.
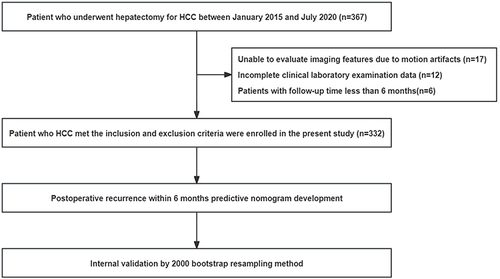
Table 1 Baseline Characteristics
Figure 2 (A) Schematic diagram; (B) Case: Male, 54 years old. On August 9, 2017, liver-specific contrast-enhanced MRI showed a solitary lesion (asterisk) in the right lobe of the liver, with a fusion nodular type of growth and multiple satellite nodules (yellow arrows) in the surrounding area. Preoperative AFP, GGT, ALP, and PT levels were 4881 ng/mL, 127 U/L, 87 U/L, and 13s, respectively. The postoperative pathological diagnosis was hepatocellular carcinoma. On January 3, 2018, liver-specific contrast-enhanced MRI showed multiple nodular lesions (red arrows) in the liver, but no obvious mass was observed in the surgical area.
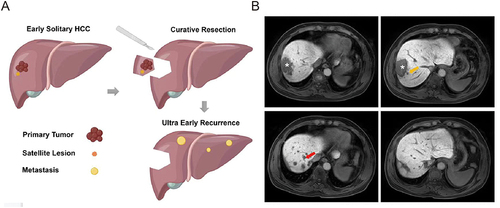
Table 2 Univariate and Multivariate Cox Regression Analysis Results for Ultra-Early Recurrence
Figure 3 (A) Nomogram for preoperative prediction of the risk of ultra-early recurrence after curative resection of early isolated hepatocellular carcinoma; (B) The area under receiver operating characteristic (ROC) curve (AUC) of the nomogram for ultra-early recurrence; (C) Calibration curves of the nomogram comparing and actual and predicted probabilities of ultra-early recurrence; (D) Decision curve analysis of the nomogram for ultra-early recurrence prediction.
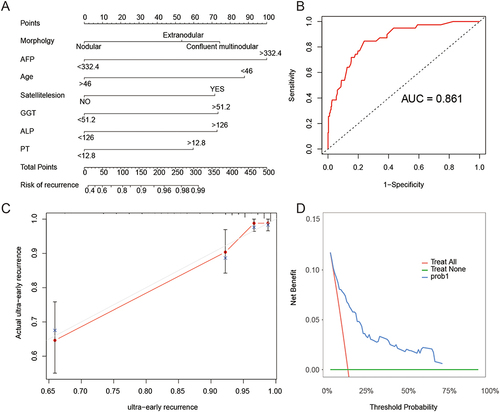
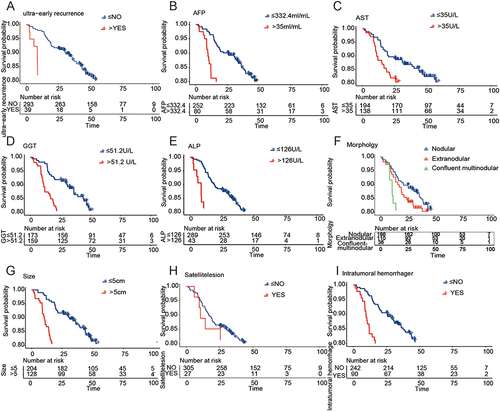
Figure 4 Factors affecting the overall survival after liver resection in patients with early solitary hepatocellular carcinoma. (A) Survival curves for patients with super-early recurrence and those without super-early recurrence. (B-I) Survival curves for AFP, AST, GGT, ALP, tumor morphology, tumor size, satellite nodules, and intratumoral hemorrhage.