Figures & data
Table 1 Demographic Characteristics of the Enrolled Patients with AHF
Figure 1 Kaplan–Meier survival curve of enrolled AHF patients, derivation cohort and validation cohort.
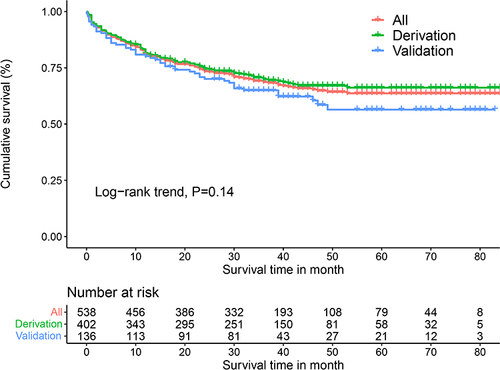
Figure 2 Selection of variables for all-cause mortality was performed using the LASSO regression plot with COX regression model. (A) LASSO model coefficient trendlines of the 57 variables (shown in Table S1) for all-cause mortality. (B) Tuning parameter (Lambda, λ) selection cross-validation error curve. Vertical lines were drawn at the optimal values given by the minimum criteria and 1-SE criteria. The right line was identified by 1-SE criteria (λ = 0.038). The parameter λ = 0.038 was selected under the 1-SE criteria. The vertical line was drawn at the value selected by 10-fold cross-validation, including optimized six non-zero coefficients proceed with further COX regression analysis.
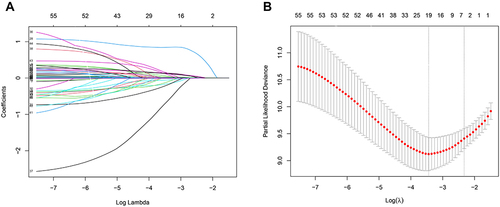
Figure 3 Forest plot with hazard ratio (HR) for the optimal prognostic variables of the final multivariable model in the derivation cohort. HRs above one indicates that a variable is positively associated with the event probability and thus negatively with survival time. A horizontal line parallel to the X-axis has a logarithmic scale represents a more precise confidence interval (95% CI).
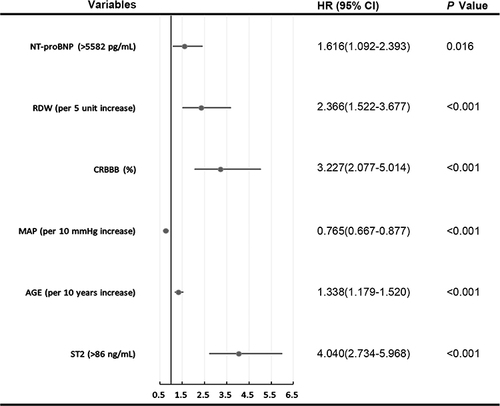
Figure 4 The BS-ACMR heart prognostic nomogram obtained from the optimal Cox model to predict 1-, 2- and 5- year overall survival for acute heart failure in derivation cohort. Each clinicopathological factor corresponds to a specific point by drawing a vertical line from that variable to the points axis. After sum of the scores for each variable located on the Total Points axis. Finally, the sum represents the probability of 1-, 2- and 5- year survival by drawing straight down to the survival axis. For example, a 24-year-old AHF patient with NT-pro BNP ≤ 5582 pg/mL, ST2 ≤ 86 ng/mL, MAP ≤ 109 mm Hg, RDW ≤ 2.82% and CRBBB, the total score will be given by 29+56+56+46+53+85 = 325, corresponding to 1-, 2-, and 5-year risks of dying of 0.049, 0.077, and 0.12, respectively. The AHF patient will accordingly have approximately 96.1%, 92.3%, and 88% survival probabilities at 1, 2, and 5 years, respectively. *P< 0.05; ***P<0.001.
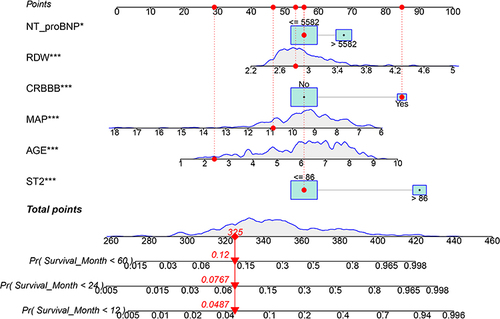
Figure 5 Discrimination analyses between derivation cohort (A) and the validation cohort (B).
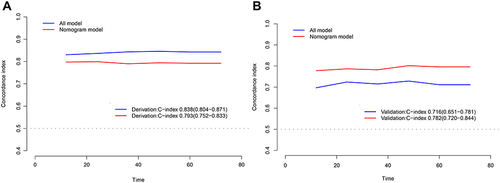
Table 2 Integrated Discrimination Improvement and Net Reclassification Improvement for All-Cause Mortality at 60 Months by Adding NT-Pro BNP and ST2 to Model
Figure 6 Calibration plot of nomogram predicted probability of 1- (A), 2- (B) and 5- (C) year all-cause mortality. Shown that the prediction model was no statistical departure with observed values.
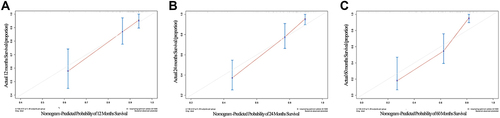
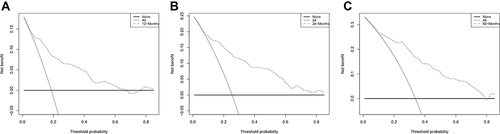
Figure 7 Decision curve of the nomogram. The black dotted line represents the nomogram. The grey solid line represents net benefit without intervention. The decision curve indicates that when the threshold probability of AHF patients of this nomogram strategies would add significant net benefit of the all-cause mortality of 1- (A), 2- (B) and 5- (C) year.