Figures & data
Figure 1 Fundus images of the left eye in case 1. Fundus photography (A) and fundus autofluorescence (B) were normal. OCT disclosed hyper-reflective segments of OPL and ONL, and associated disruption of ellipsoid, interdigitation zones, and RPE layers on the nasal macular area ((C), red box). No flow defects were observed in the superficial (D)/intermediate (E)/deep (F) retinal capillary plexuses and choroidal capillary plexus (G) on OCTA. One week after oral prednisone administration OPL and ONL hyper-reflectivity mildly faded with definable ellipsoid, interdigitation zones, and retinal pigment epithelium (RPE) layers ((H), red box). Six weeks later only slight irregularity of ellipsoid, interdigitation zones and RPE layers persisted on OCT ((I), red box).
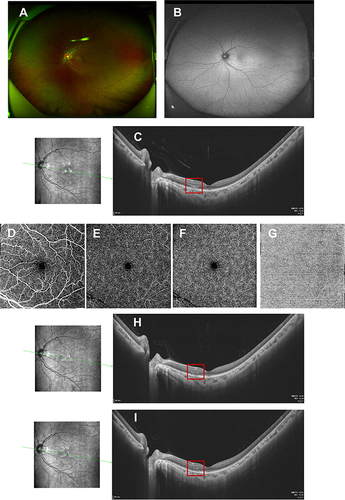
Figure 2 Fundus images of the left eye in case 2. Fundus photography (A) was normal. OCT disclosed hyper-reflective segment of OPL and ONL, and associated disruption of ellipsoid, interdigitation zones, and RPE layers on the nasal ((B), red box) and upper macular ((C), red box). No flow defects in the superficial (D)/intermediate (E)/deep (F) retinal capillary plexuses and choroidal capillary plexus (G) on OCTA. Three weeks after oral prednisone administration, hyper-reflectivity of the OPL and ONL completely faded with definable ellipsoid, interdigitation zones, and RPE layers both on the nasal ((H), red box) and upper ((I), red box) macular on OCT. Six weeks later only slight irregularity of ellipsoid, interdigitation zones, and RPE layers persisted on OCT, on the nasal ((J), red box) and upper ((K), red box) macular areas.
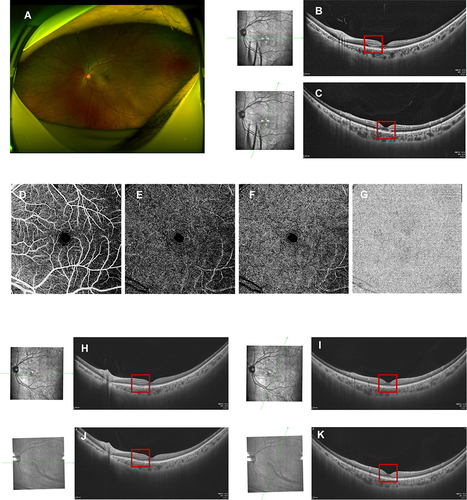
Figure 3 Fundus images of the left eye in case 3. Fundus photography (A) was normal. A para-foveal hyper-reflective segment of the OPL and ONL, with associated disruption of ellipsoid, interdigitation zones, and RPE layers on OCT ((B), red box). No flow defects in the superficial (C)/intermediate (D)/deep (E) retinal capillary plexuses and choroidal capillary plexus (F) on OCTA. Three days after oral prednisone administration, hyper-reflectivity of the OPL and ONL mildly faded on OCT ((G), red box). Ten days later, hyper-reflectivity faded with definable ellipsoid, interdigitation zones, and RPE layers on the OCT ((H), red box). A tiny segmental discontinuity of ellipsoid, interdigitation zones, and RPE layers persisted on OCT at the 4-week visit ((I), red box) and 7-week visit ((J), red box).
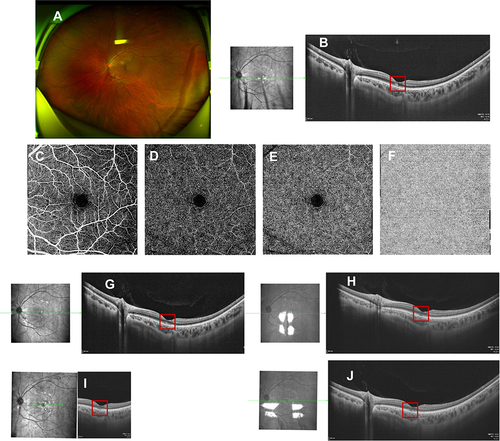
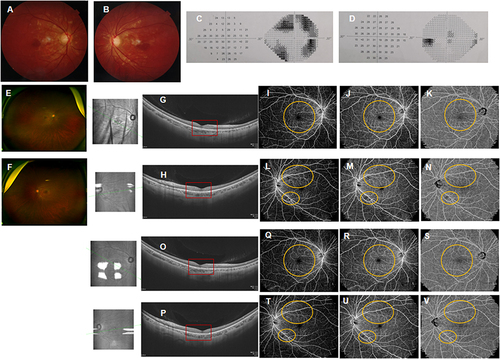
Figure 4 Fundus images of both eyes in case 4. Initial fundus photography revealed white-yellow lesions in the posterior retina in both eyes (Right: (A), Left: (B), photocopy from local records). The 30–2 visual field test showed visual defects on nasal and temporal fields in the right eye (C), while it was normal in the left eye ((D), photocopy from local records). At presentation, fundus photography showed reduced white-yellow lesions (Right: (E), Left: (F)) and OCT scan disclosed hyper-reflective segment of the OPL and ONL in the fovea of both eyes, also with associated disruption of ellipsoid, interdigitation zones, and RPE layers (Right: (G), Left: (H), red box). OCTA showed perfusion defects in the superficial (I and L)/deep (J and M) retinal capillary plexuses, also in the choroidal capillary plexus (K and N) on wide field OCTA in both eyes (Right: (I–K). Left: (L–N), yellow circle). Hyper-reflectivity of the OPL and ONL slightly faded (Right: (O), Left: (P), red box) one week after oral prednisone administration, as observed in OCT. Superficial (Q and T)/deep (R and U) retinal capillary defects, and choroidal (S and V) capillary defects slightly resolved on OCTA (Right: (Q–S). Left: (T–V), yellow circle).