
Figures & data
Figure 1 A review of all COVID-19-related documentation discussed at RVH’s EOC committee between March-June, 2020, as well as COVID-19 documentation provided by external partners between February-June, 2020, identified recurrent themes critical to RVH’s pandemic response.
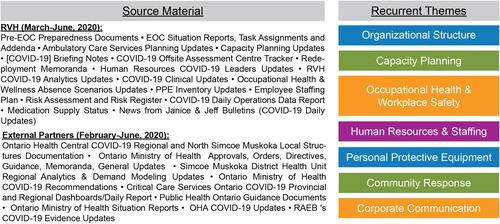
Figure 2 RVH’s modified EOC structure is based on a traditional IMS system, comprised of interconnected command staff (green) and general staff (blue), with clinical operations divided into clinical care, clinical support, and capacity planning. Non-traditional sections were added to fulfil local pandemic needs, including corporate communications and resource leads.
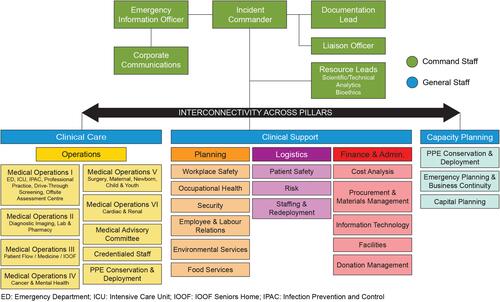
Figure 3 A robust capacity plan guided by the principles of design thinking permitted RVH to expand its level 3 critical care capacity from 16 beds to 105 beds in 5–12 weeks, along with an additional 334 standard beds and 300 cots (not shown), as required.
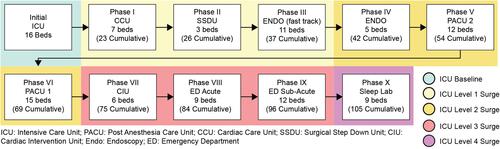
Figure 4 A structured, five-step workforce planning cycle was established to identify and fulfil clinical staffing requirements, as well as cleaning staff, environmental services aides, and other staff essential to meeting workforce demands and upholding patient safety. This framework was further supported by strategies and actions to source, recruit, onboard, train, and develop staff.
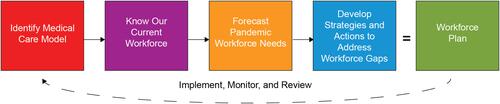
Figure 5 The pandemic response unit (PRU) is a 70-bed, 8250 square-foot, four season, fully-functioning modular field hospital located in RVH’s parking lot and connected to the health centre by an enclosed walkway. The PRU is professionally staffed and fully equipped regional asset to assist RVH and partner hospitals facing capacity challenges during the COVID-19 pandemic. Of note, the PRU is not a unit for COVID patients, but for medically stable inpatients with an estimated stay of 3–5 days.
