Figures & data
Figure 1 Distal femur radiograph.
Notes: Anteroposterior radiograph of the distal femur of a 23-year-old woman presenting with enlargement of distal thigh with occasional pain. Image shows a large mineralized mass.

Figure 2 Distal femur MRI.
Note: Coronal T1-weighted magnetic resonance image shows marrow replacement of distal femur and a soft tissue mass extending beyond the bone cortex.
Abbreviation: MRI, magnetic resonance imaging.
Abbreviation: MRI, magnetic resonance imaging.

Figure 3 Distal femur CT biopsy.
Notes: Image-guided biopsy was carried out under computed tomography guidance by the musculoskeletal radiologist following discussion at the Multidisciplinary Sarcoma Tumor Board. The needle trajectory, arrived at upon discussion with the surgical team, is evident.
Abbreviation: CT, computed tomograhpy.
Abbreviation: CT, computed tomograhpy.
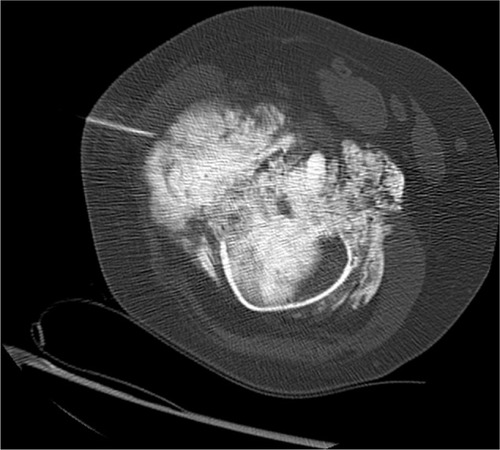
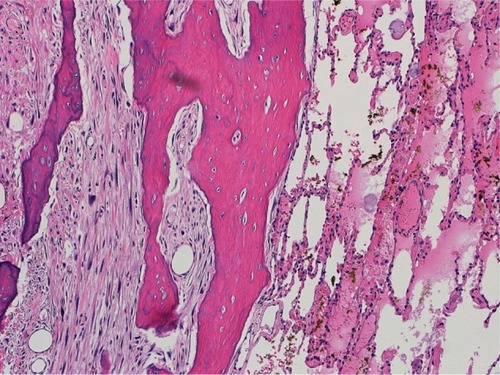
Figure 4 Distal femur biopsy photomicrograph.
Notes: Photomicrograph of the initial core needle biopsy depicts features of low grade parosteal osteosarcoma. The neoplastic stroma in between bone trabeculae contained spindle cells with small uniform nuclei (arrow). Histology was presented at the Multidisciplinary Sarcoma Tumor Board, and recommendation was made for distal femoral resection (hematoxylin and eosin, 400×).
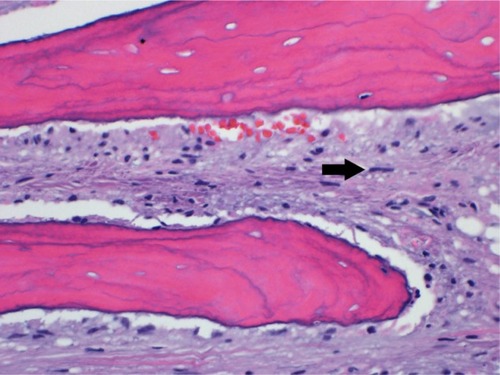
Table 1 Multidisciplinary team approach to sarcoma treatment
Figure 5 Postoperative radiograph.
Note: Anteroposterior radiograph following distal femoral resection and endoprosthetic reconstruction by the orthopedic oncologist.

Figure 6 Distal femur final pathology photomicrograph.
Notes: Evaluation of the complete resection specimen by the musculoskeletal pathologist showed areas of higher grade osteosarcoma. These areas were much more cellular and had larger more atypical nuclei and increased mitotic activity (arrow) compared with the initial biopsy. Following review at the Multidisciplinary Sarcoma Tumor Board, the consensus recommendation for postoperative multiagent chemotherapy was made based on clinical, radiographic, and histologic review (hematoxylin and eosin, 400×).
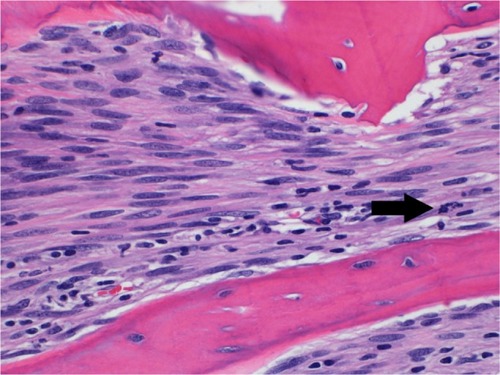
Figure 7 CT thorax.
Notes: Following a disease-free interval of 18 months following surgery, a lung nodule was identified on routine postoperative surveillance, as seen on this axial computed tomography image. The patient’s care was again reviewed and the consensus recommendation made for second-line chemotherapy followed by resection of the pulmonary nodule with video-assisted thoracic surgery.
Abbreviation: CT, computed tomograhpy.
Abbreviation: CT, computed tomograhpy.

Figure 8 Metastasectomy photomicrograph.
Notes: Photomicrograph confirms metastatic sarcoma in the lungs resected by the thoracic surgeon. Review of viable disease by the multidisciplinary team led to enrollment of the patient into a clinical trial with an experimental agent. A second metastasectomy procedure 1 year later with wedge resections for pulmonary disease showed focal high grade dedifferentiation but with margins negative. Experimental chemotherapy on clinical trial was resumed. One year following metastasectomy, the patient remains alive without measurable disease, continuing under the care of the multidisciplinary team, 4½ years after initial diagnosis (hematoxylin and eosin, 100×).