
Figures & data
Figure 1 BoNT-A in migraine: putative mechanisms of action.
Notes: BoNT-A induces a chemical denervation, which reverts peripheral sensitization and, indirectly, central sensitization. BoNT-A injection in pericranial muscles blocks neuropeptide (substance P, CGRP) and neurotransmitter (Glu) release from peripheral trigeminal sensory nerve endings. BoNT-A also deranges the translocation to nerve ending plasma membrane of NMDA glutamate receptor, TRPV1 and P2X3 purinoreceptors. A still controversial hypothesis suggests that BoNT-A could also act centrally, being transferred to second-order nociceptive neurons via retrograde axonal transport and transcytosis.
Abbreviations: BoNT-A, onabotulinum toxin A; CGRP, calcitonin gene-related peptide; Glu, glutamate; NMDA, N-methy-D-aspartate; TRPV1, transient receptor potential vanilloid 1; NKA, Neurokinin A; SP, substance P; SNARE, soluble n-ethylmaleimide-sensitive factor attachment protein receptor; SNAP-25, synaptosomal-associated protein of 25 kDa.
Abbreviations: BoNT-A, onabotulinum toxin A; CGRP, calcitonin gene-related peptide; Glu, glutamate; NMDA, N-methy-D-aspartate; TRPV1, transient receptor potential vanilloid 1; NKA, Neurokinin A; SP, substance P; SNARE, soluble n-ethylmaleimide-sensitive factor attachment protein receptor; SNAP-25, synaptosomal-associated protein of 25 kDa.
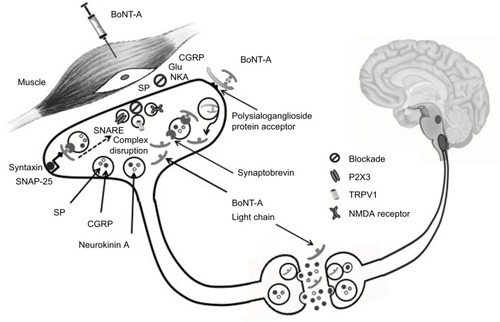
Figure 2 Imploding/ocular pain might be a consequence of the trigemino-autonomic reflex activation: a hypothesis.
Notes: In 1/3 of migraineurs, an overactivation of the TN – causing a more strictly unilateral and severe headache located along the areas of cutaneous distribution of the ophthalmic branch (1) – induces both central sensitization (allodynia and photophobia) and the activation of the efferent arm of the trigeminal-autonomic reflex (2). Activated preganglionic parasympathetic fibers originating in the SSN exit the brainstem via the seventh cranial nerve (VII), traverse the GG and synapse in the SPG with postsynaptic neurons innervating cranial and conjunctival vessels, lacrimal glands and nasal mucosa, triggering UAs (ocular/periocular vasodilation and edema, lacrimation and rhinorrhea) (3). UAs would activate extracranial nociceptors (4), being responsible for imploding/periocular pain characteristics, and would in turn amplify trigeminal afferent firing (5), further perpetuating the vicious cycle.
Abbreviations: TN, trigeminal nerve; SSN, superior salivatory nucleus; GG, geniculate ganglion; SPG, sphenopalatine; UAs, unilateral autonomic symptom; TCC, trigeminocervical complex; TG, trigeminal ganglion.
Abbreviations: TN, trigeminal nerve; SSN, superior salivatory nucleus; GG, geniculate ganglion; SPG, sphenopalatine; UAs, unilateral autonomic symptom; TCC, trigeminocervical complex; TG, trigeminal ganglion.
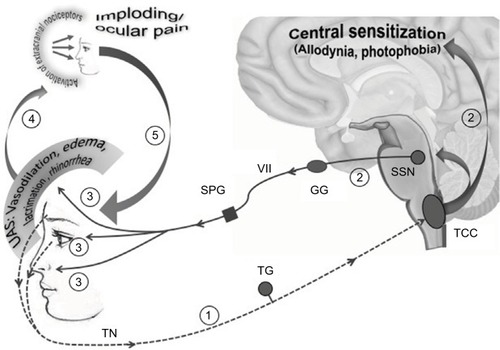
Table 1 BoNT-A in CM treatment: issues to be addressed