Figures & data
Figure 1 A concise scheme illustrating the balance of epithelial-to-mesenchymal transition markers in sarcomatoid carcinoma sustained by up- and down-regulation of different molecules and gene alterations governing the tumor cell cellular program.
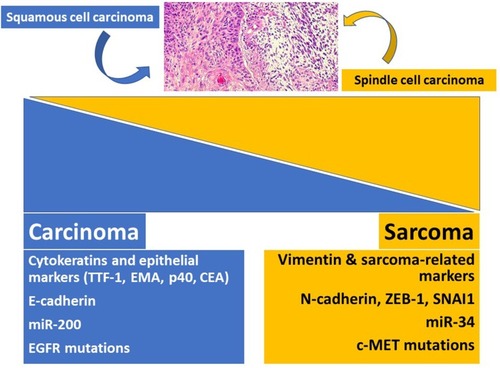
Figure 2 Bronchoscopy showing a whitish polypoid lesion consistent with carcinosarcoma at histology.
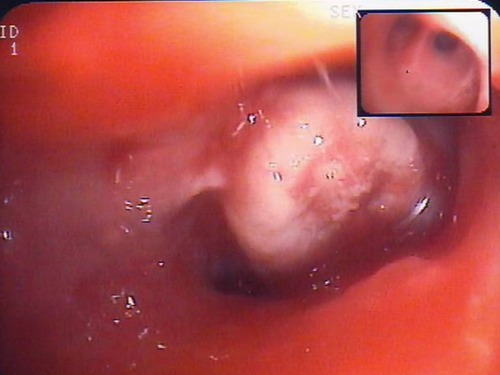
Figure 3 Sarcomatoid carcinoma of the right lung presenting as a large, rounded mass at chest X-rays.
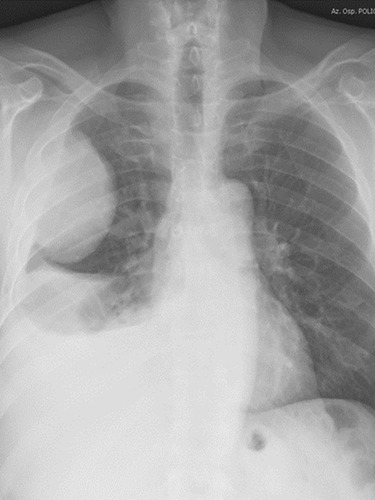
Figure 4 Sarcomatoid carcinoma appearing as a large nodular lesion of the right upper lobe with relatively well-defined margins at computed tomography of the thorax.
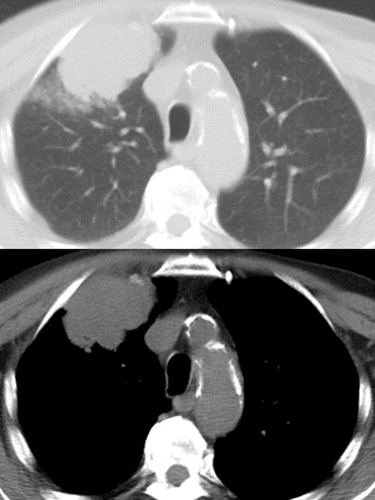
Figure 5 Macroscopic appearance of a pulmonary carcinosarcoma consisting of a large (>10 cm), whitish and fleshy mass with well-demarcated tumor border and heterogenous cut surface.

Table 1 Characteristics Possibly Indicating a Patient with Pulmonary Sarcomatoid Carcinoma
Table 2 Diagnostic Criteria of Pulmonary Sarcomatoid Carcinomas
Figure 6 Histology of pleomorphic carcinoma revealing an adenocarcinoma (at the top) intermingled with neoplastic spindle cell component (A). Pure spindle cell carcinoma (B) consisting of a dense and irregular proliferation of atypical spindle cells with marked nuclear atypia and eosinophilic cytoplasm.
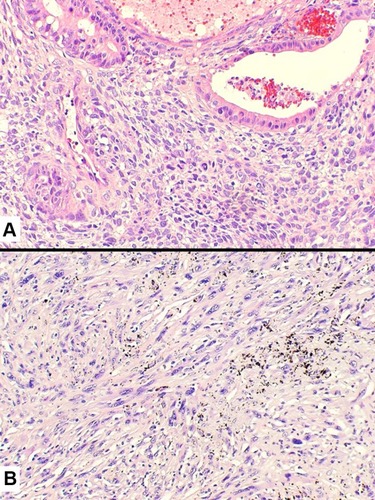
Figure 7 Tumor cell infiltration of a medium-sized vessel wall by spindle cell carcinoma (A) also highlighted by the expression of pan-cytokeratins (clone CAM5.2) (B).
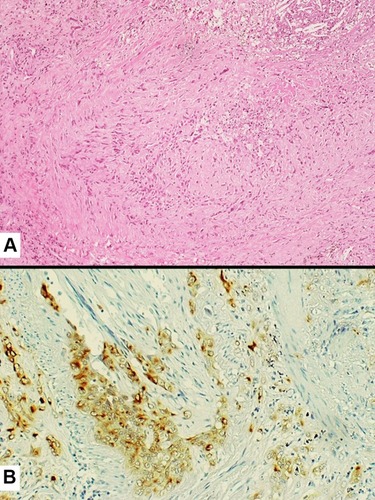
Figure 8 Inflammatory-type spindle cell carcinoma showing a chaotic proliferation of spindle cells with prominent nucleoli into collagenized stroma with a mixed inflammatory infiltrate (A). Positive staining with pan-cytokeratins (clone AE1/AE3) revealing the epithelial/carcinoma differentiation of spindle elements (B).
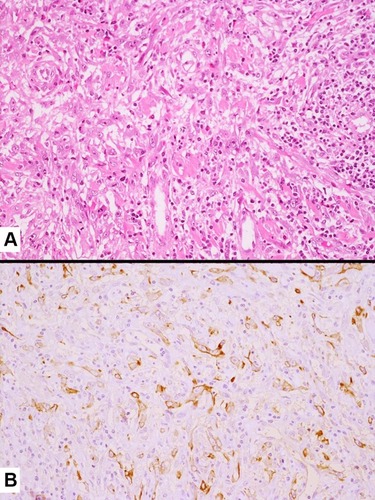
Figure 9 Histology of giant cell carcinoma showing a discohesive proliferation of bizarre, large tumor cells and the presence of sparse inflammatory infiltrates focally involving the cytoplasm of tumor cells (emperipolesis) (A). Carcinosarcoma consisting of a poorly differentiated squamous cell carcinoma (right) with a heterologous chondrosarcomatous component (left) (B).
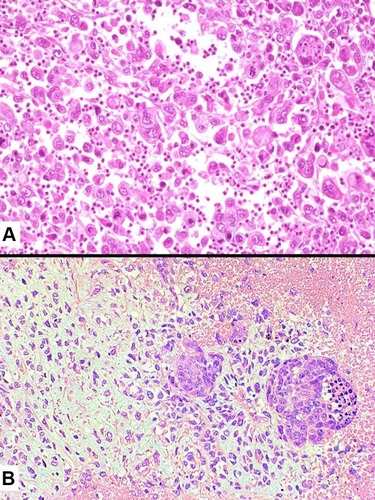
Figure 10 Pulmonary blastoma showing a minor component of well-differentiated adenocarcinoma (top) admixed with an undifferentiated blastematous component.
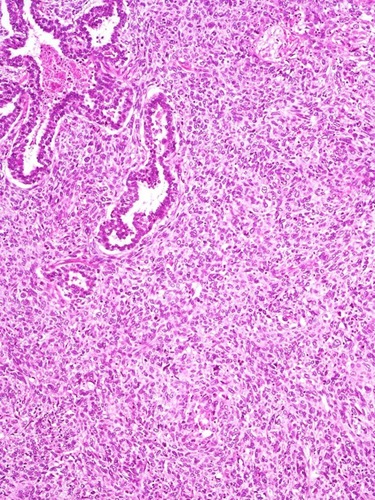
Table 3 Ancillary Techniques in Differential Diagnosis Between Pulmonary Sarcomatoid Carcinoma and Mimicking Tumors
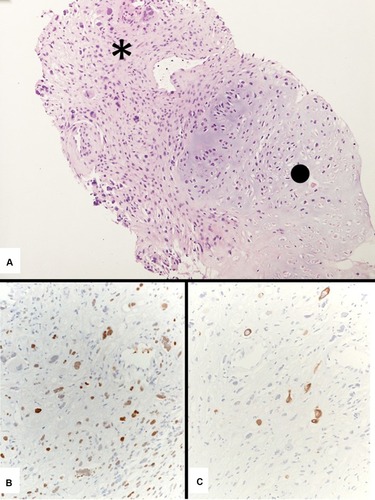
Figure 11 A generous transthoracic biopsy consistent with a carcinosarcoma showing an undifferentiated spindle cell carcinoma (asterisk) and a heterologous chondrosarcoma (dot) (A). Immunostains with pan-cytokeratins (clone MNF116) (B) and TTF-1 (clone 8G7G3/1) (C) demonstrate the epithelial adenocarcinomatous differentiation of the spindle cell component.